Klawitter Jost, Bendrick-Peart Jamie, Rudolph Birgit, Beckey Virginia, Klawitter Jelena, Haschke Manuel, Rivard Christopher, Chan Laurence, Leibfritz Dieter, Christians Uwe, Schmitz Volker
Departments of Anesthesiology and Nephrology, University of Colorado, Denver, Colorado, USA.
Chem Res Toxicol. 2009 Jan;22(1):118-28. doi: 10.1021/tx800253x.
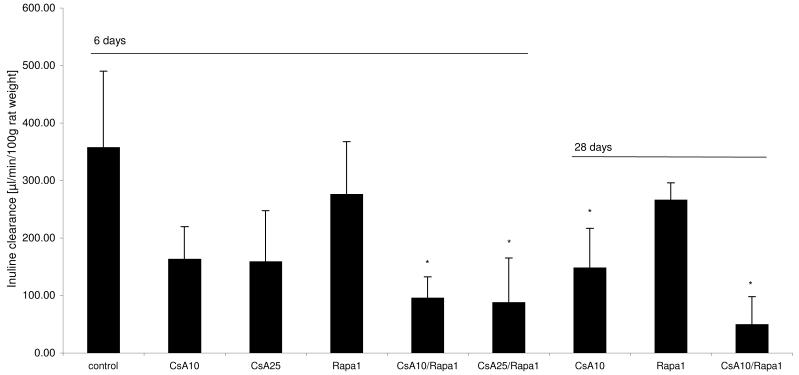
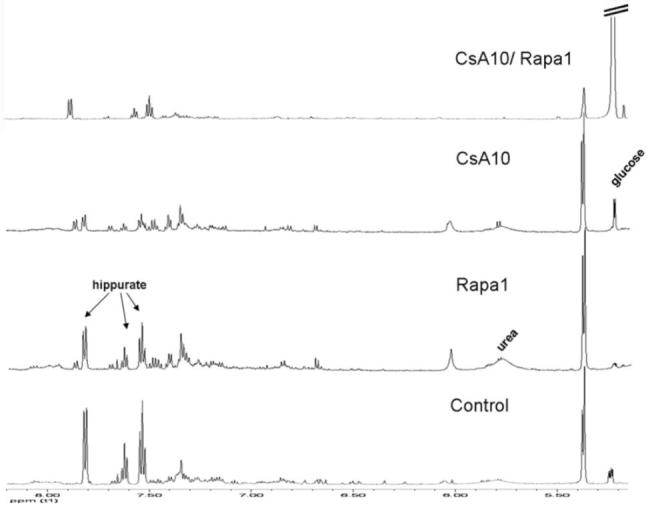
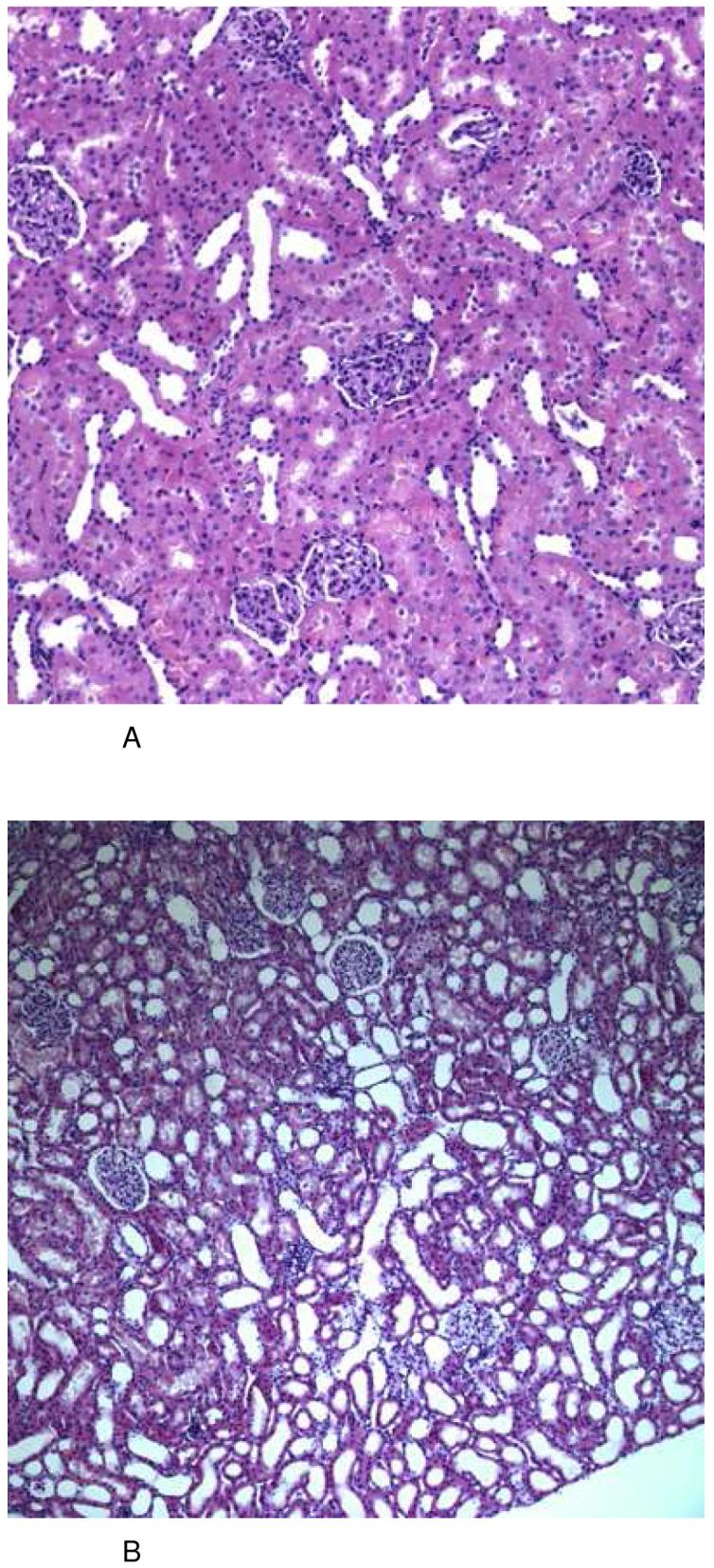
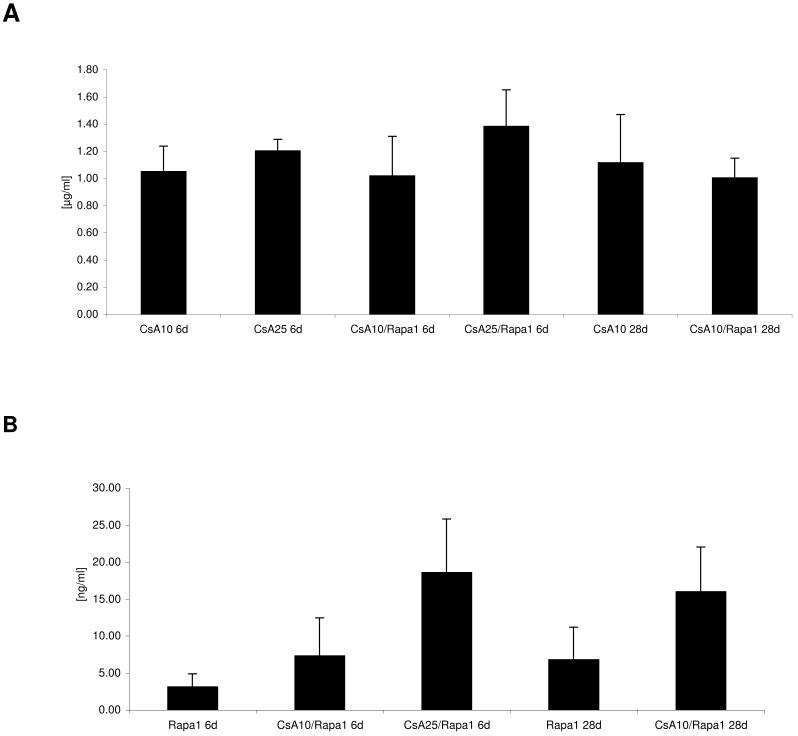
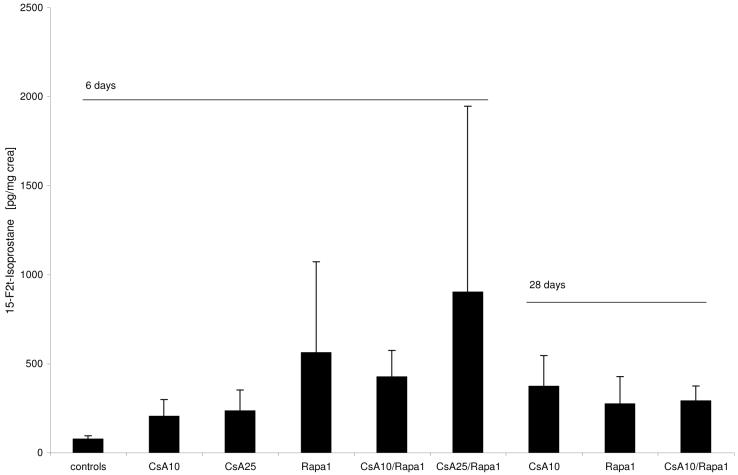
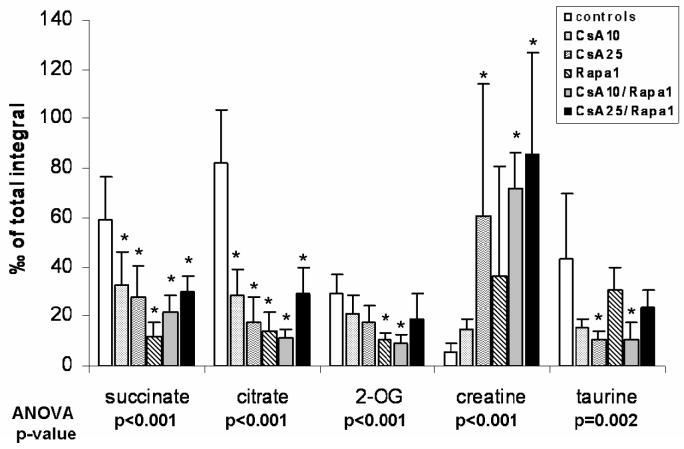
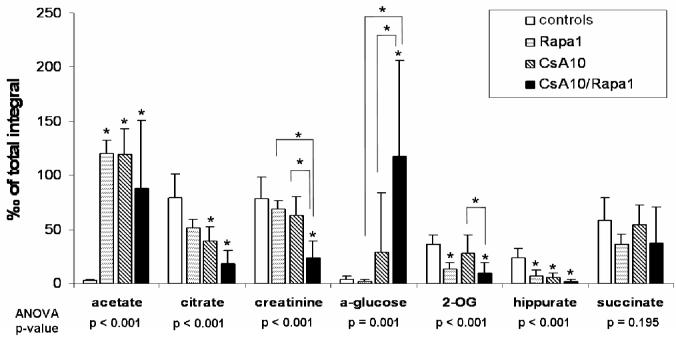
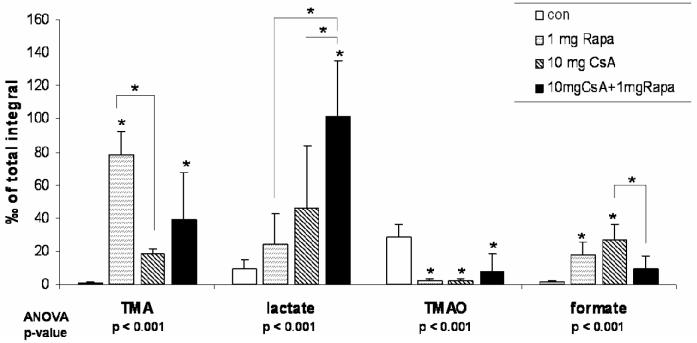
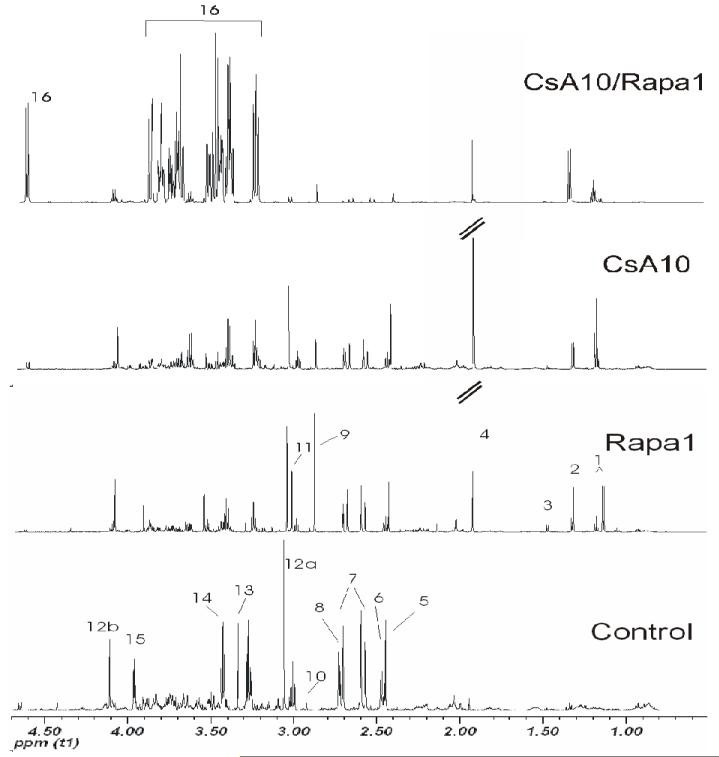
The clinical use of the immunosuppressant calcineurin inhibitor cyclosporine is limited by its nephrotoxicity. This is enhanced when combined with the immunosuppressive mTOR inhibitor sirolimus. Nephrotoxicity of both drugs is not yet fully understood. The goal was to gain more detailed mechanistic insights into the time-dependent effects of cyclosporine and sirolimus on the rat kidney by using a comprehensive approach including metabolic profiling in urine ((1)H NMR spectroscopy), kidney histology, kidney function parameters in plasma, measurement of glomerular filtration rates, the oxidative stress marker 15-F(2t)-isoprostane in urine, and immunosuppressant concentrations in blood and kidney. Male Wistar rats were treated with vehicle (controls), cyclosporine (10/25 mg/kg/day), and/or sirolimus (1 mg/kg/day) by oral gavage once daily for 6 and 28 days. Twenty-eight day treatment led to a decrease of glomerular filtration rates (cyclosporine, -59%; sirolimus, -25%). These were further decreased when both drugs were combined (-86%). Histology revealed tubular damage after treatment with cyclosporine, which was enhanced when sirolimus was added. No other part of the kidney was affected. (1)H NMR spectroscopy analysis of urine (day 6) revealed time-dependent changes of 2-oxoglutarate, citrate, and succinate concentrations. In combination with increased urine isoprostane concentrations, these changes indicated oxidative stress. After 28 days of cyclosporine treatment, urine metabonomics shifted to patterns typical for proximal tubular damage with reduction of Krebs cycle intermediates and trimethylamine-N-oxide concentrations, whereas acetate, lactate, trimethylamine, and glucose concentrations increased. Again, sirolimus enhanced these negative effects. Our results indicate that cyclosporine and/or sirolimus induce damage of the renal tubular system. This is reflected by urine metabolite patterns, which seem to be more sensitive than currently used clinical kidney function markers such as creatinine concentrations in serum. Metabolic profiling in urine may provide the basis for the development of toxicodynamic monitoring strategies for immunosuppressant nephrotoxicity.
免疫抑制剂环孢素的临床应用受到其肾毒性的限制。当与免疫抑制性mTOR抑制剂西罗莫司联合使用时,这种毒性会增强。两种药物的肾毒性尚未完全明确。目标是通过采用综合方法,包括尿液代谢物谱分析(¹H NMR光谱法)、肾脏组织学、血浆中的肾功能参数、肾小球滤过率测量、尿液中氧化应激标志物15-F(2t)-异前列腺素以及血液和肾脏中免疫抑制剂浓度,更详细地了解环孢素和西罗莫司对大鼠肾脏的时间依赖性影响。雄性Wistar大鼠通过每日一次口服灌胃给予赋形剂(对照组)、环孢素(10/25 mg/kg/天)和/或西罗莫司(1 mg/kg/天),持续6天和28天。28天的治疗导致肾小球滤过率下降(环孢素,-59%;西罗莫司,-25%)。当两种药物联合使用时,肾小球滤过率进一步下降(-86%)。组织学显示,环孢素治疗后肾小管受损,添加西罗莫司后损伤加剧。肾脏的其他部分未受影响。尿液的¹H NMR光谱分析(第6天)显示2-氧代戊二酸、柠檬酸和琥珀酸浓度随时间变化。这些变化与尿液中异前列腺素浓度升高相结合,表明存在氧化应激。环孢素治疗28天后,尿液代谢组学转变为近端肾小管损伤的典型模式,三羧酸循环中间体和氧化三甲胺浓度降低,而乙酸盐、乳酸盐、三甲胺和葡萄糖浓度升高。同样,西罗莫司增强了这些负面影响。我们的结果表明,环孢素和/或西罗莫司会导致肾小管系统损伤。这通过尿液代谢物模式得以体现,尿液代谢物模式似乎比目前使用的临床肾功能标志物(如血清肌酐浓度)更敏感。尿液代谢物谱分析可能为免疫抑制剂肾毒性的毒效动力学监测策略的开发提供基础。