University of Alabama at Birmingham, 1530 3rd Ave South, CH-19, Ste-219, Birmingham AL 35294-2041, United States.
Int J Cardiol. 2009 May 29;134(3):330-5. doi: 10.1016/j.ijcard.2008.12.089.
Chronic kidney disease (CKD) and diabetes mellitus (DM) are common comorbidities in heart failure (HF) and each is associated with poor outcomes. However, the effects of multimorbidity related to having both CKD and DM compared to CKD alone have not been well studied in a propensity-matched population of chronic HF patients.
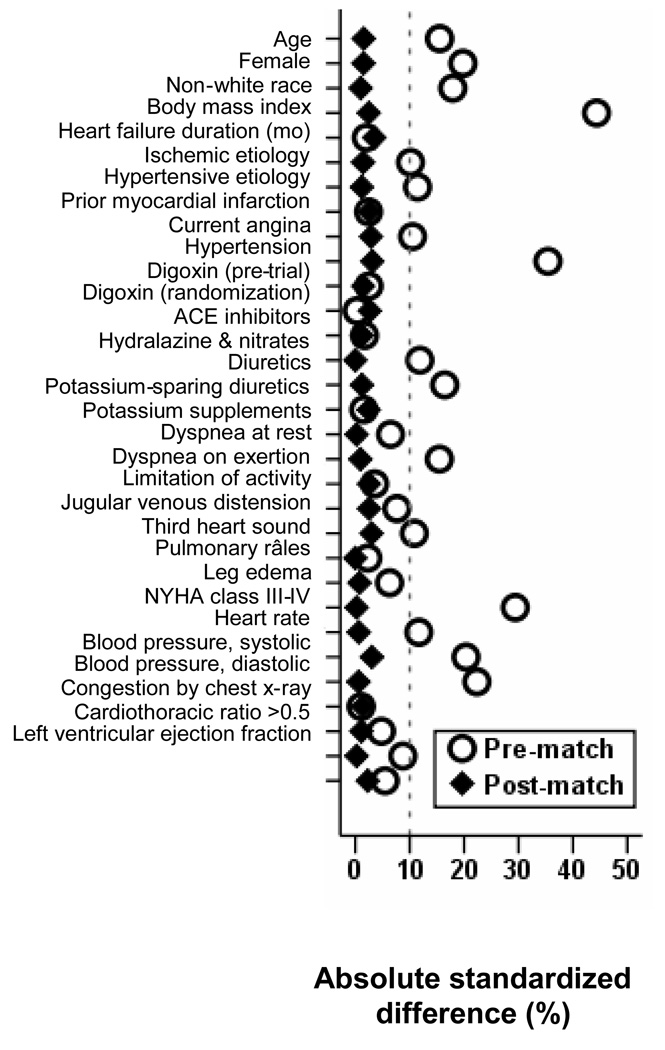
Of the 7788 ambulatory chronic HF patients in the Digitalis Investigation Group trial, 3527 had CKD, of whom 1095 had DM. Based on the absence or presence of DM, patients were categorized CKD-only and CKD-DM, respectively. Propensity scores for CKD-DM were calculated for each patient and were used to match 987 pairs of CKD-only and CKD-DM patients. Hazard ratios (HR) and 95% confidence intervals (CI) comparing CKD-DM patients with CKD-only patients were estimated using matched Cox regression models.
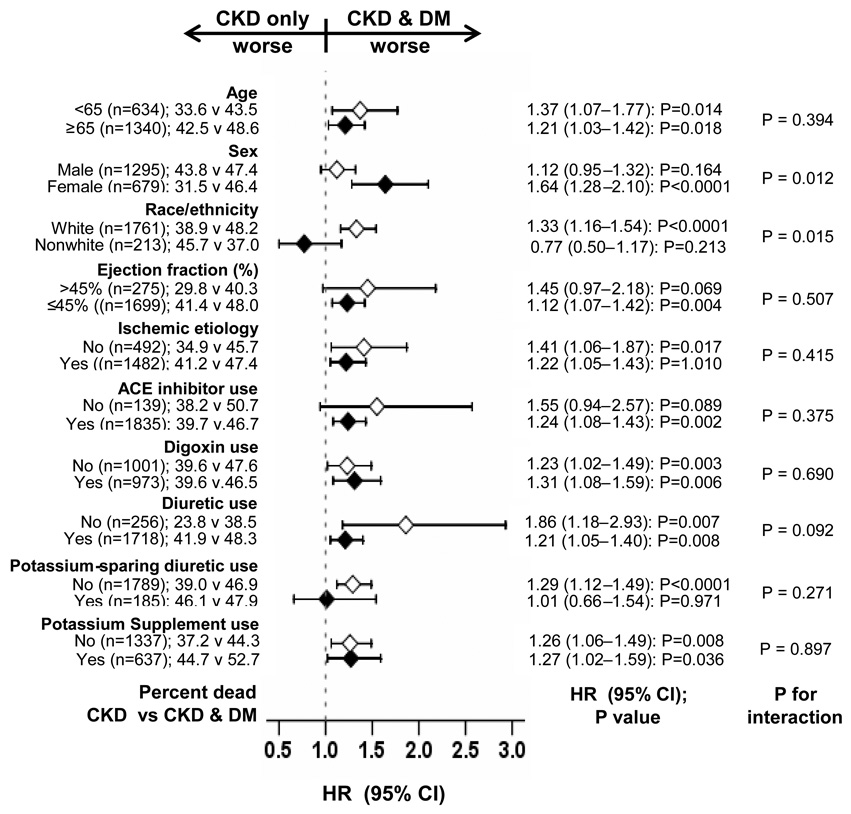
All-cause mortality occurred in 47.0% (rate, 1783/10,000 person-years of follow-up) of CKD-DM patients and 39.6% (rate, 1414/10,000 person-years) of CKD-only patients (HR when CKD-DM is compared with CKD-only, 1.25; 95%-CI, 1.07-1.46; p=0.006). All-cause hospitalization occurred in 75.4% (rate, 5710/10,000 person-years) and 67.8% (rate, 4213/10,000 person-years) of CKD-DM and CKD-only patients respectively (HR, 1.32; 95%-CI, 1.15-1.52; p<0.0001). Respective HR and 95%-CI for other outcomes were: cardiovascular mortality (1.27; 1.06-1.52; p=0.009), HF mortality (1.34; 1.04-1.72; p=0.025); cardiovascular hospitalization (1.29; 1.12-1.49; p=0.001) and HF hospitalization (1.37; 1.16-1.63; p<0.0001).
Compared with comorbidity due to CKD alone, multimorbidity with CKD and DM was associated with poor outcomes in chronic HF patients.
慢性肾脏病(CKD)和糖尿病(DM)是心力衰竭(HF)的常见合并症,两者均与不良结局相关。然而,在患有慢性 HF 的倾向匹配人群中,与仅患有 CKD 相比,同时患有 CKD 和 DM 的多合并症的影响尚未得到充分研究。
在 Digitalis Investigation Group 试验的 7788 名门诊慢性 HF 患者中,有 3527 名患有 CKD,其中 1095 名患有 DM。根据是否存在 DM,患者分别归类为仅 CKD 和 CKD-DM。为每位患者计算 CKD-DM 的倾向评分,并使用该评分匹配 987 对 CKD-仅和 CKD-DM 患者。使用匹配的 Cox 回归模型估计 CKD-DM 患者与 CKD-仅患者相比的风险比(HR)和 95%置信区间(CI)。
在 CKD-DM 患者中,全因死亡率为 47.0%(发生率为 1783/10,000 人年随访),在 CKD-仅患者中为 39.6%(发生率为 1414/10,000 人年)(与 CKD-仅相比,当 CKD-DM 被比较时,HR 为 1.25;95%CI,1.07-1.46;p=0.006)。全因住院治疗分别发生在 CKD-DM 患者(发生率为 5710/10,000 人年)和 CKD-仅患者(发生率为 4213/10,000 人年)中 75.4%和 67.8%(HR,1.32;95%CI,1.15-1.52;p<0.0001)。其他结果的相应 HR 和 95%CI 为:心血管死亡率(1.27;1.06-1.52;p=0.009),HF 死亡率(1.34;1.04-1.72;p=0.025);心血管住院率(1.29;1.12-1.49;p=0.001)和 HF 住院率(1.37;1.16-1.63;p<0.0001)。
与仅 CKD 引起的合并症相比,患有 CKD 和 DM 的合并症与慢性 HF 患者的不良结局相关。