Flierl Michael A, Beauchamp Kathryn M, Bolles Gene E, Moore Ernest E, Stahel Philip F
Department of Orthopaedic Surgery, Denver Health Medical Center, University of Colorado School of Medicine, 777 Bannock Street, Denver, CO 80204, USA.
Patient Saf Surg. 2009 Feb 25;3(1):4. doi: 10.1186/1754-9493-3-4.
Pyogenic spondylodiscitis represents a potentially life-threatening condition. Due to the low incidence, evidence-based surgical recommendations in the literature are equivocal, and the treatment modalities remain controversial.
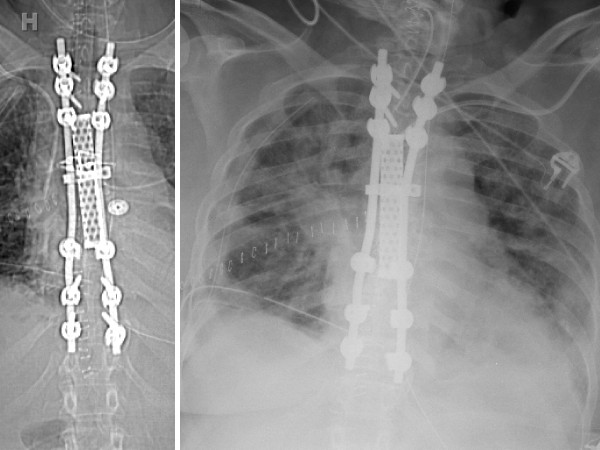
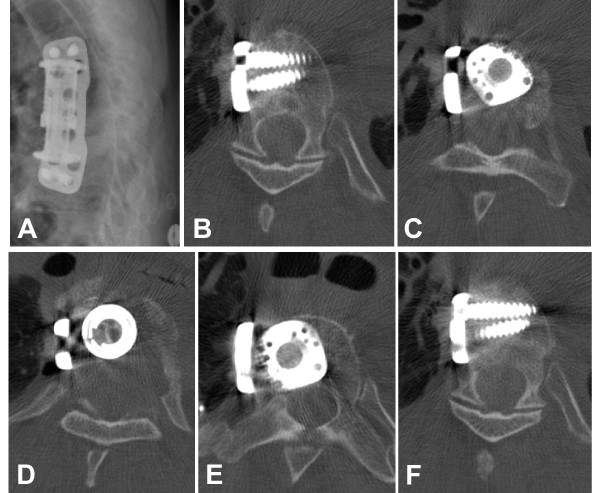
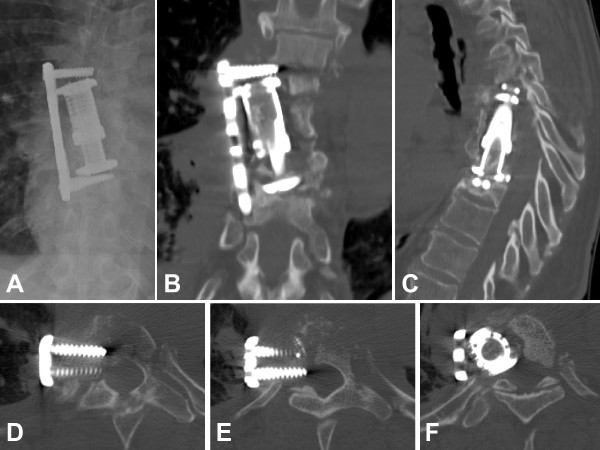
A 59 year-old patient presented with a history of thoracic spondylodiscitis resistant to antibiotic treatment for 6 weeks, progressive severe back pain, and a new onset of bilateral lower extremity weakness. Clinically, the patient showed a deteriorating spastic paraparesis of her lower extremities. An emergent MRI revealed a kyphotic wedge compression fracture at T7/T8 with significant spinal cord compression, paravertebral and epidural abscess, and signs of myelopathy. The patient underwent surgical debridement with stabilization of the anterior column from T6-T9 using an expandable titanium cage, autologous bone graft, and an anterolateral locking plate. The patient recovered well under adjunctive antibiotic treatment. She presented again to the emergency department 6 months later, secondary to a repeat fall, with acute paraplegia of the lower extremities and radiographic evidence of failure of fixation of the anterior T-spine. She underwent antero-posterior revision fixation with hardware removal, correction of kyphotic malunion, evacuation of a recurrent epidural abscess, decompression of the spinal canal, and 360 degrees fusion from T2-T11. Despite the successful salvage procedure, the patient deteriorated in the postoperative phase, when she developed multiple complications including pneumonia, acute respiratory distress syndrome, bacterial meningitis, abdominal compartment syndrome, followed by septic shock with multiple organ failure and a lethal outcome within two weeks after revision surgery.
This catastrophic example of a lethal outcome secondary to failure of anterior column fixation for pyogenic thoracic spondylodiscitis underlines the notion that surgical strategies for the infected spine must be aimed at achieving absolute stability by a 360 degrees fusion. This aggressive - albeit controversial - concept allows for an adequate infection control by adjunctive antibiotics and reduces the imminent risk of a secondary loss of fixation due to compromises in initial fixation techniques.
化脓性脊椎椎间盘炎是一种潜在的危及生命的疾病。由于发病率低,文献中基于证据的手术建议并不明确,治疗方式仍存在争议。
一名59岁患者,有胸椎椎间盘炎病史,抗生素治疗6周无效,伴有进行性严重背痛和新发双侧下肢无力。临床上,患者下肢痉挛性轻瘫逐渐加重。急诊MRI显示T7/T8处有后凸楔形压缩骨折,伴有明显脊髓受压、椎旁和硬膜外脓肿以及脊髓病迹象。患者接受了手术清创,使用可扩张钛笼、自体骨移植和前外侧锁定钢板对T6 - T9的前柱进行稳定。在辅助抗生素治疗下,患者恢复良好。6个月后,她因再次跌倒再次就诊于急诊科,出现下肢急性截瘫,影像学显示胸椎前路固定失败。她接受了前后路翻修固定,包括取出内固定物、矫正后凸畸形愈合、清除复发性硬膜外脓肿、椎管减压以及T2 - T11的360度融合。尽管挽救手术成功,但患者在术后病情恶化,出现了多种并发症,包括肺炎、急性呼吸窘迫综合征、细菌性脑膜炎、腹腔间隔室综合征,随后发展为感染性休克伴多器官功能衰竭,在翻修手术后两周内死亡。
这个化脓性胸椎椎间盘炎前路固定失败导致致命后果的灾难性案例强调了这样一个观点,即感染性脊柱的手术策略必须旨在通过360度融合实现绝对稳定。这种激进的——尽管有争议——概念通过辅助抗生素能够充分控制感染,并降低由于初始固定技术不完善而导致继发固定失败的紧迫风险。