Crivaro Valeria, Di Popolo Anna, Caprio Alessandro, Lambiase Antonietta, Di Resta Mario, Borriello Tonia, Scarcella Alda, Triassi Maria, Zarrilli Raffaele
Dipartimento di Scienze Mediche Preventive, Sezione di Igiene, Università Federico II, Napoli, Italy.
BMC Infect Dis. 2009 May 22;9:70. doi: 10.1186/1471-2334-9-70.
Pseudomonas aeruginosa, a non-fermentative, gram-negative rod, is responsible for a wide variety of clinical syndromes in NICU patients, including sepsis, pneumonia, meningitis, diarrhea, conjunctivitis and skin infections. An increased number of infections and colonisations by P. aeruginosa has been observed in the neonatal intensive care unit (NICU) of our university hospital between 2005 and 2007.
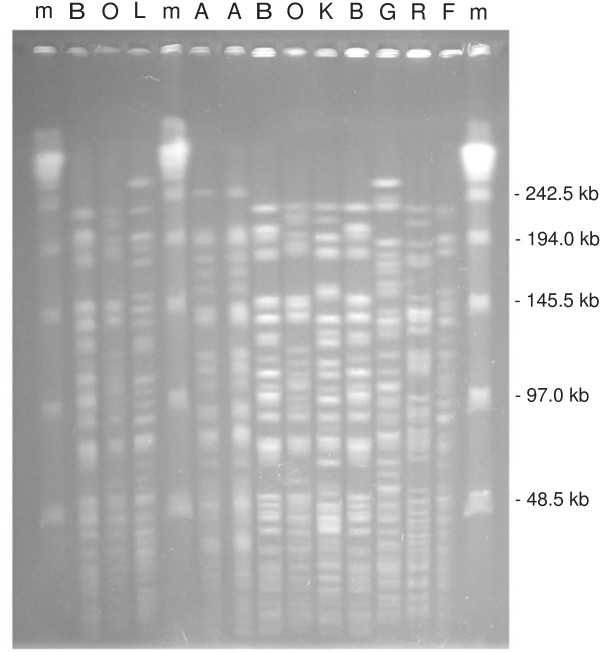
Hand disinfection compliance before and after an educational programme on hand hygiene was evaluated. Identification of microrganisms was performed using conventional methods. Antibiotic susceptibility was evaluated by MIC microdilution. Genotyping was performed by PFGE analysis.
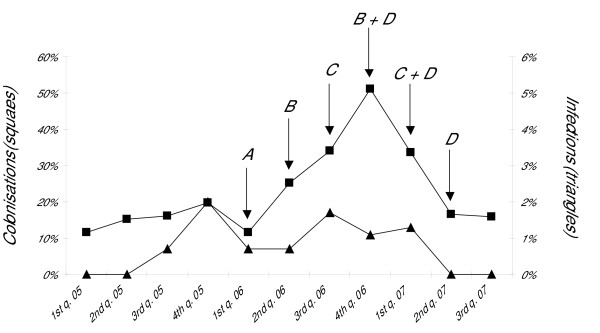
The molecular epidemiology of Pseudomonas aeruginosa in the NICU of the Federico II University hospital (Naples, Italy) and the infection control measures adopted to stop the spreading of P. aeruginosa in the ward were described. From July 2005 to June 2007, P. aeruginosa was isolated from 135 neonates and caused severe infections in 11 of them. Macrorestriction analysis of clinical isolates from 90 neonates identified 20 distinct genotypes, one major PFGE type (A) being isolated from 48 patients and responsible for 4 infections in 4 of them, four other distinct recurrent genotypes being isolated in 6 to 4 patients. Seven environmental strains were isolated from the hand of a nurse and from three sinks on two occasions, two of these showing PFGE profiles A and G identical to two clinical isolates responsible for infection. The successful control of the outbreak was achieved through implementation of active surveillance of healthcare-associated infections in the ward together with environmental microbiological sampling and an intense educational programme on hand disinfection among the staff members.
P. aeruginosa infections in the NICU were caused by the cross-transmission of an epidemic clone in 4 neonates, and by the selection of sporadic clones in 7 others. An infection control programme that included active surveillance and strict adherence to hand disinfection policies was effective in controlling NICU-acquired infections and colonisations caused by P. aeruginosa.
铜绿假单胞菌是一种非发酵革兰氏阴性杆菌,可导致新生儿重症监护病房(NICU)患者出现多种临床综合征,包括败血症、肺炎、脑膜炎、腹泻、结膜炎和皮肤感染。2005年至2007年期间,在我校医院的新生儿重症监护病房中,观察到铜绿假单胞菌感染和定植数量有所增加。
对手卫生教育计划前后的手部消毒依从性进行评估。使用常规方法进行微生物鉴定。通过MIC微量稀释法评估抗生素敏感性。通过PFGE分析进行基因分型。
描述了意大利那不勒斯费德里科二世大学医院新生儿重症监护病房中铜绿假单胞菌的分子流行病学以及为阻止该菌在病房传播而采取的感染控制措施。2005年7月至2007年6月,从135名新生儿中分离出铜绿假单胞菌,其中11人发生严重感染。对90名新生儿临床分离株的宏观限制性分析确定了20种不同的基因型,一种主要的PFGE型(A)从48名患者中分离出,导致其中4人发生4起感染,另外4种不同的复发性基因型分别从6至4名患者中分离出。两次从一名护士的手部和三个水槽中分离出7株环境菌株,其中两株的PFGE图谱A和G与两株导致感染的临床分离株相同。通过在病房实施医疗保健相关感染的主动监测、环境微生物采样以及对工作人员进行强化手部消毒教育计划,成功控制了疫情。
新生儿重症监护病房中的铜绿假单胞菌感染,4例由流行克隆的交叉传播引起,另外7例由散发性克隆的选择引起。包括主动监测和严格遵守手部消毒政策的感染控制计划,对于控制新生儿重症监护病房获得性铜绿假单胞菌感染和定植有效。