Frye Robert L, August Phyllis, Brooks Maria Mori, Hardison Regina M, Kelsey Sheryl F, MacGregor Joan M, Orchard Trevor J, Chaitman Bernard R, Genuth Saul M, Goldberg Suzanne H, Hlatky Mark A, Jones Teresa L Z, Molitch Mark E, Nesto Richard W, Sako Edward Y, Sobel Burton E
N Engl J Med. 2009 Jun 11;360(24):2503-15. doi: 10.1056/NEJMoa0805796. Epub 2009 Jun 7.
Optimal treatment for patients with both type 2 diabetes mellitus and stable ischemic heart disease has not been established.
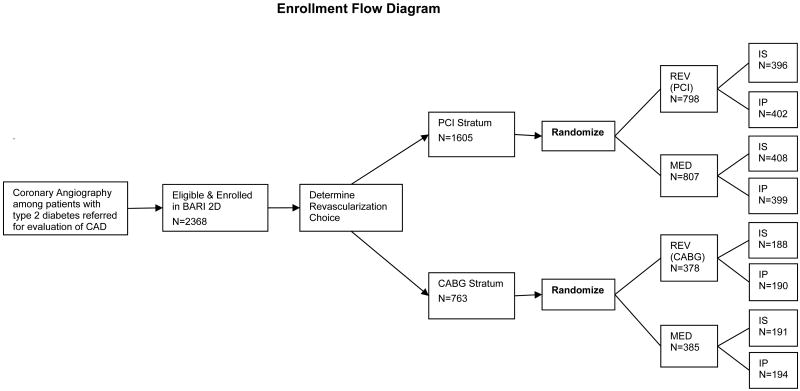
We randomly assigned 2368 patients with both type 2 diabetes and heart disease to undergo either prompt revascularization with intensive medical therapy or intensive medical therapy alone and to undergo either insulin-sensitization or insulin-provision therapy. Primary end points were the rate of death and a composite of death, myocardial infarction, or stroke (major cardiovascular events). Randomization was stratified according to the choice of percutaneous coronary intervention (PCI) or coronary-artery bypass grafting (CABG) as the more appropriate intervention.
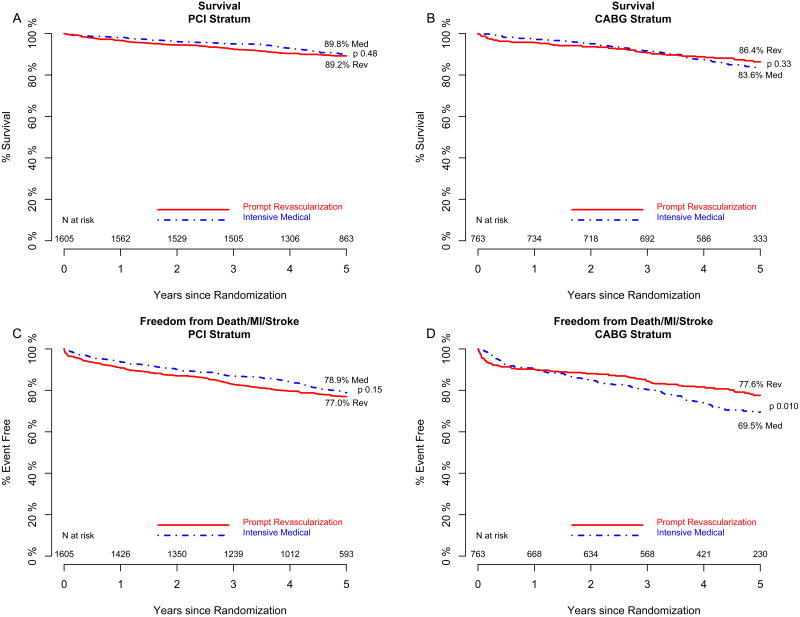
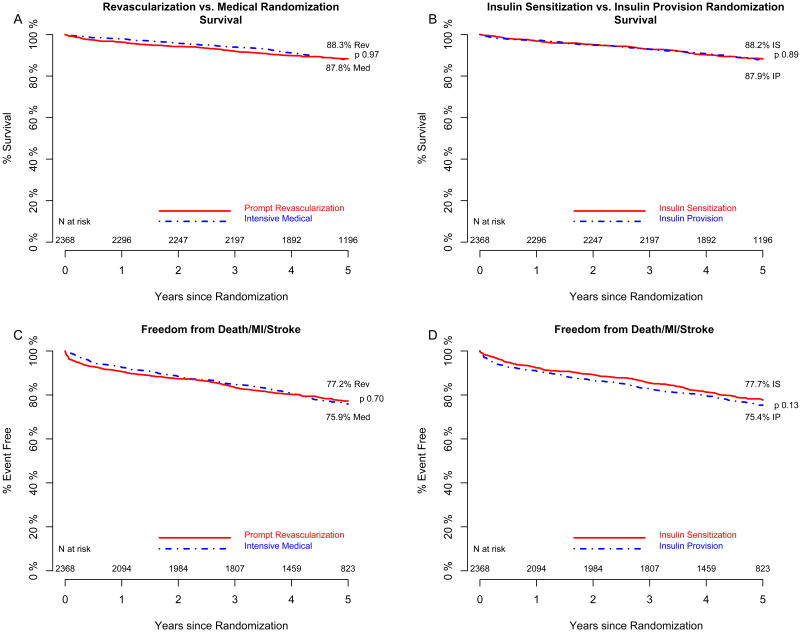
At 5 years, rates of survival did not differ significantly between the revascularization group (88.3%) and the medical-therapy group (87.8%, P=0.97) or between the insulin-sensitization group (88.2%) and the insulin-provision group (87.9%, P=0.89). The rates of freedom from major cardiovascular events also did not differ significantly among the groups: 77.2% in the revascularization group and 75.9% in the medical-treatment group (P=0.70) and 77.7% in the insulin-sensitization group and 75.4% in the insulin-provision group (P=0.13). In the PCI stratum, there was no significant difference in primary end points between the revascularization group and the medical-therapy group. In the CABG stratum, the rate of major cardiovascular events was significantly lower in the revascularization group (22.4%) than in the medical-therapy group (30.5%, P=0.01; P=0.002 for interaction between stratum and study group). Adverse events and serious adverse events were generally similar among the groups, although severe hypoglycemia was more frequent in the insulin-provision group (9.2%) than in the insulin-sensitization group (5.9%, P=0.003).
Overall, there was no significant difference in the rates of death and major cardiovascular events between patients undergoing prompt revascularization and those undergoing medical therapy or between strategies of insulin sensitization and insulin provision. (ClinicalTrials.gov number, NCT00006305.)
2型糖尿病合并稳定型缺血性心脏病患者的最佳治疗方案尚未确定。
我们将2368例2型糖尿病合并心脏病患者随机分组,分别接受强化药物治疗下的即刻血运重建或单纯强化药物治疗,以及胰岛素增敏治疗或胰岛素补充治疗。主要终点为死亡率以及死亡、心肌梗死或中风的复合终点(主要心血管事件)。随机分组根据经皮冠状动脉介入治疗(PCI)或冠状动脉旁路移植术(CABG)作为更合适的干预措施的选择进行分层。
5年后,血运重建组(88.3%)和药物治疗组(87.8%,P = 0.97)之间的生存率无显著差异,胰岛素增敏组(88.2%)和胰岛素补充组(87.9%,P = 0.89)之间的生存率也无显著差异。各组主要心血管事件的无事件发生率也无显著差异:血运重建组为77.2%,药物治疗组为75.9%(P = 0.70),胰岛素增敏组为77.7%,胰岛素补充组为75.4%(P = 0.13)。在PCI分层中,血运重建组和药物治疗组的主要终点无显著差异。在CABG分层中,血运重建组的主要心血管事件发生率(22.4%)显著低于药物治疗组(30.5%,P = 0.01;分层与研究组之间的交互作用P = 0.002)。各组的不良事件和严重不良事件总体相似,尽管胰岛素补充组(9.2%)的严重低血糖发生率高于胰岛素增敏组(5.9%,P = 0.003)。
总体而言,接受即刻血运重建的患者与接受药物治疗的患者之间,以及胰岛素增敏策略与胰岛素补充策略之间,在死亡率和主要心血管事件发生率方面无显著差异。(ClinicalTrials.gov编号,NCT00006305。)