Department of Internal Medicine, Washington University School of Medicine, St. Louis, MO.
Cardiovascular Division, Washington University School of Medicine, St. Louis, MO.
J Am Heart Assoc. 2017 Sep 13;6(9):e005946. doi: 10.1161/JAHA.117.005946.
In the BARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes) trial, randomization of diabetic patients with stable ischemic heart disease to insulin provision (IP) therapy, as opposed to insulin sensitization (IS) therapy, resulted in biochemical evidence of impaired fibrinolysis but no increase in adverse clinical outcomes. We hypothesized that the prothrombotic effect of IP therapy in combination with the hypercoagulable state induced by active smoking would result in an increased risk of myocardial infarction (MI).
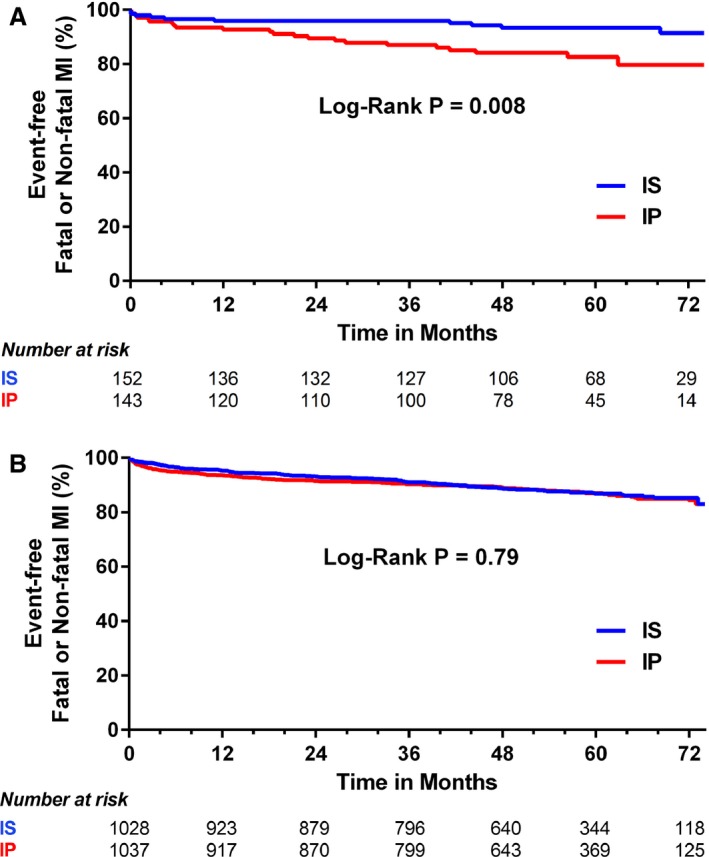
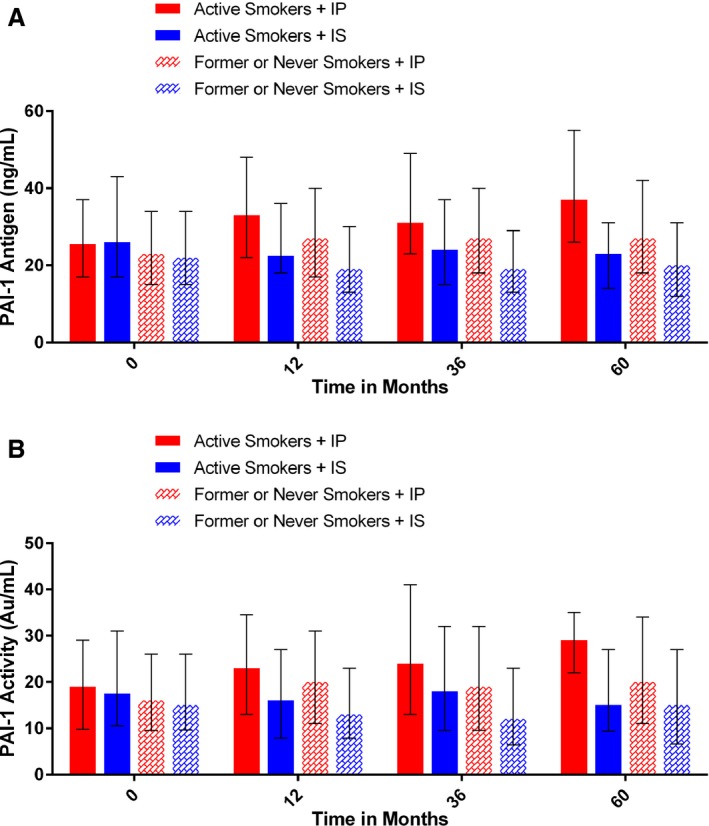
We analyzed BARI 2D patients who were active smokers randomized to IP or IS therapy. The primary end point was fatal or nonfatal MI. PAI-1 (plasminogen activator inhibitor 1) activity was analyzed at 1, 3, and 5 years. Of 295 active smokers, MI occurred in 15.4% randomized to IP and in 6.8% randomized to IS over the 5.3 years (=0.023). IP therapy was associated with a 3.2-fold increase in the hazard of MI compared with IS therapy (hazard ratio: 3.23; 95% confidence interval, 1.43-7.28; =0.005). Baseline PAI-1 activity (19.0 versus 17.5 Au/mL, =0.70) was similar in actively smoking patients randomized to IP or IS therapy. However, IP therapy resulted in significantly increased PAI-1 activity at 1 year (23.0 versus 16.0 Au/mL, =0.001), 3 years (24.0 versus 18.0 Au/mL, =0.049), and 5 years (29.0 versus 15.0 Au/mL, =0.004) compared with IS therapy.
Among diabetic patients with stable ischemic heart disease who were actively smoking, IP therapy was independently associated with a significantly increased hazard of MI. This finding may be explained by higher PAI-1 activity in active smokers treated with IP therapy.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00006305.
在 BARI 2D(旁路血管成形术再血管化调查 2 型糖尿病)试验中,将稳定型缺血性心脏病的糖尿病患者随机分为胰岛素提供(IP)治疗组和胰岛素增敏(IS)治疗组,结果显示前者的生物化学证据表明纤溶受损,但并未增加不良临床结局。我们假设 IP 治疗的促血栓形成作用与主动吸烟引起的高凝状态相结合,会导致心肌梗死(MI)的风险增加。
我们分析了 BARI 2D 试验中同时为活跃吸烟者并被随机分配至 IP 或 IS 治疗组的患者。主要终点是致死性或非致死性 MI。在 1、3 和 5 年时分析 PAI-1(纤溶酶原激活物抑制剂 1)活性。在 295 名活跃吸烟者中,15.4%随机分配至 IP 组的患者和 6.8%随机分配至 IS 组的患者在 5.3 年内发生 MI(=0.023)。与 IS 治疗相比,IP 治疗与 MI 风险增加 3.2 倍相关(危险比:3.23;95%置信区间,1.43-7.28;=0.005)。在随机分配至 IP 或 IS 治疗的活跃吸烟者中,基线 PAI-1 活性(19.0 与 17.5 Au/mL,=0.70)相似。然而,与 IS 治疗相比,IP 治疗在 1 年(23.0 与 16.0 Au/mL,=0.001)、3 年(24.0 与 18.0 Au/mL,=0.049)和 5 年(29.0 与 15.0 Au/mL,=0.004)时,PAI-1 活性显著增加。
在患有稳定型缺血性心脏病且为活跃吸烟者的糖尿病患者中,IP 治疗与 MI 风险显著增加独立相关。这一发现可能可以通过 IP 治疗组中较高的 PAI-1 活性来解释。