Alexander Andrea, Rehders Alexander, Raffel Andreas, Poremba Christopher, Knoefel Wolfram T, Eisenberger Claus F
Klinik für Allgemein-, Viszeral- und Kinderchirurgie, Universitätsklinikum Düsseldorf, Germany.
World J Surg Oncol. 2009 Jun 26;7:56. doi: 10.1186/1477-7819-7-56.
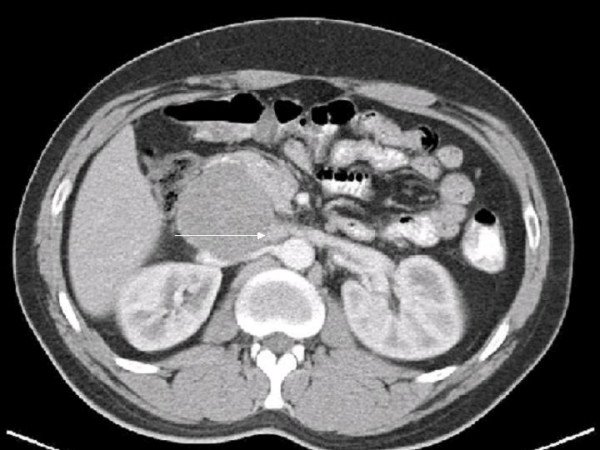
Vascular leiomyosarcoma are rare tumors typically originating from the inferior vena cava (IVC). Due to nonspecific clinical signs most tumors are diagnosed at advanced stages. Complete surgical resection remains the only potential curative therapeutic option. Surgical strategy is particularly influenced by the level of the IVC affected. Due to the topographic relation to the renal veins level-II involvement of the IVC raises special surgical challenges with respect to the maintenance of venous outflow.
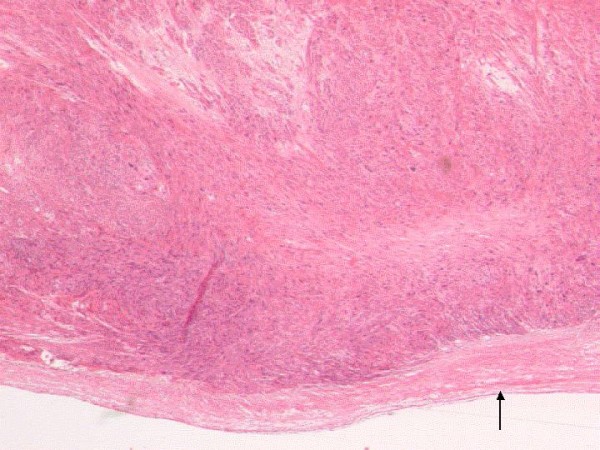
We herein report two cases of leiomyosarcoma of the IVC with successful en bloc resection and individualized caval reconstruction. One patient presented with a large intramural and intraluminal mass and received a complete circumferential resection. Reconstruction was performed by graft replacement of the caval segment affected. The other patient displayed a predominantly extraluminal tumor growth and underwent semicircumferential resection of the IVC including the confluence of the left renal vein. In this case vascular reconstruction was performed by cavoplasty and reinsertion of the left renal vein into the proximal portion of the IVC. Resection margins of both patients were tumor free and no clinical signs of venous insufficiency of the lower extremity occurred.
This paper presents two cases of successfully managed leiomyosarcomas of the vena cava and exemplifies two different options for vascular reconstruction in level II sarcomas and includes a thorough review of the literature.
血管平滑肌肉瘤是一种罕见肿瘤,通常起源于下腔静脉(IVC)。由于临床症状不具特异性,大多数肿瘤在晚期才被诊断出来。完整的手术切除仍然是唯一可能治愈的治疗选择。手术策略尤其受到IVC受累水平的影响。由于与肾静脉的解剖关系,IVC的二级受累在维持静脉流出方面带来了特殊的手术挑战。
我们在此报告两例IVC平滑肌肉瘤患者,成功进行了整块切除并进行了个体化的腔静脉重建。一名患者表现为巨大的壁内和腔内肿块,接受了完整的环形切除。通过移植置换受影响的腔静脉段进行重建。另一名患者主要表现为腔外肿瘤生长,接受了IVC的半环形切除,包括左肾静脉汇合处。在这种情况下,通过腔静脉成形术和将左肾静脉重新插入IVC近端进行血管重建。两名患者的切除边缘均无肿瘤,且未出现下肢静脉功能不全的临床症状。
本文介绍了两例成功治疗的腔静脉平滑肌肉瘤病例,举例说明了二级肉瘤血管重建的两种不同选择,并对文献进行了全面回顾。