Department of Epidemiology, University of Washington, Seattle, Washington 98195-7920, USA.
Alcohol Clin Exp Res. 2009 Oct;33(10):1671-89. doi: 10.1111/j.1530-0277.2009.01004.x. Epub 2009 Jul 1.
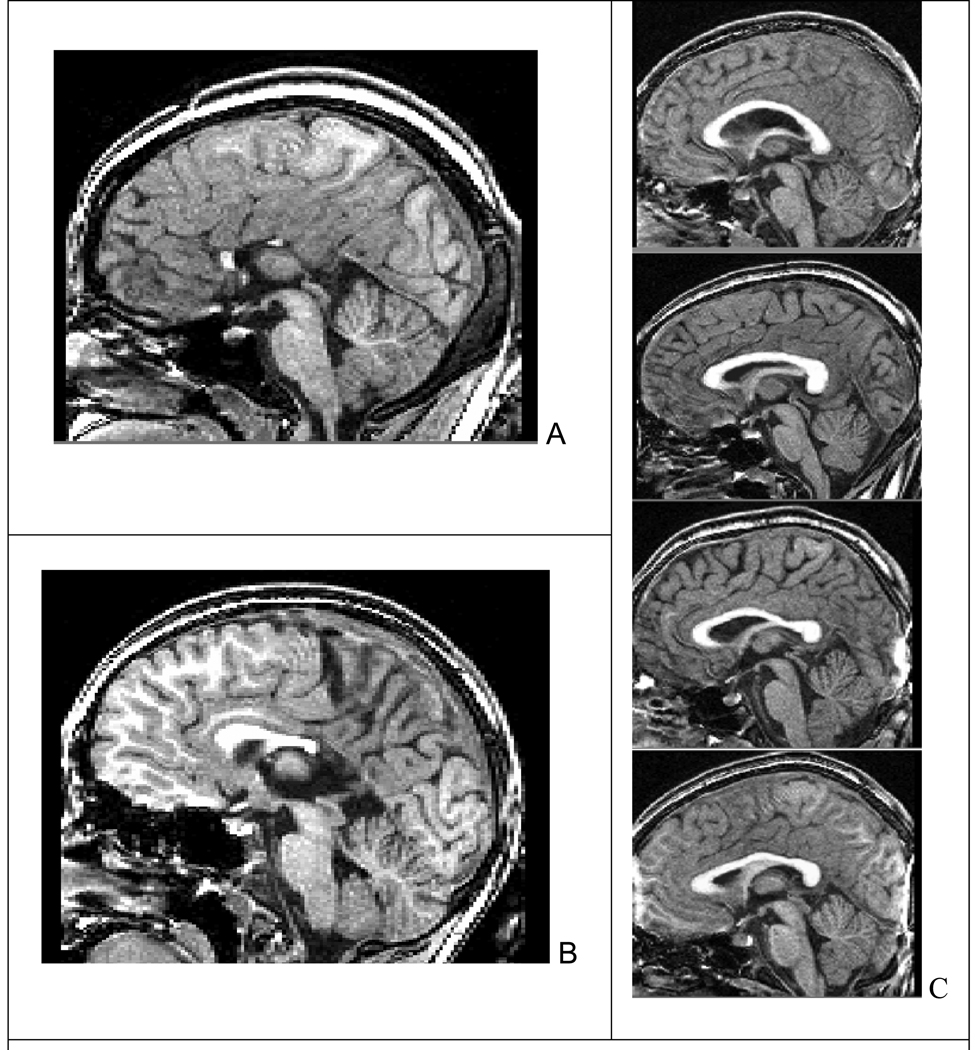
Magnetic resonance (MR) technology offers noninvasive methods for in vivo assessment of neuroabnormalities.
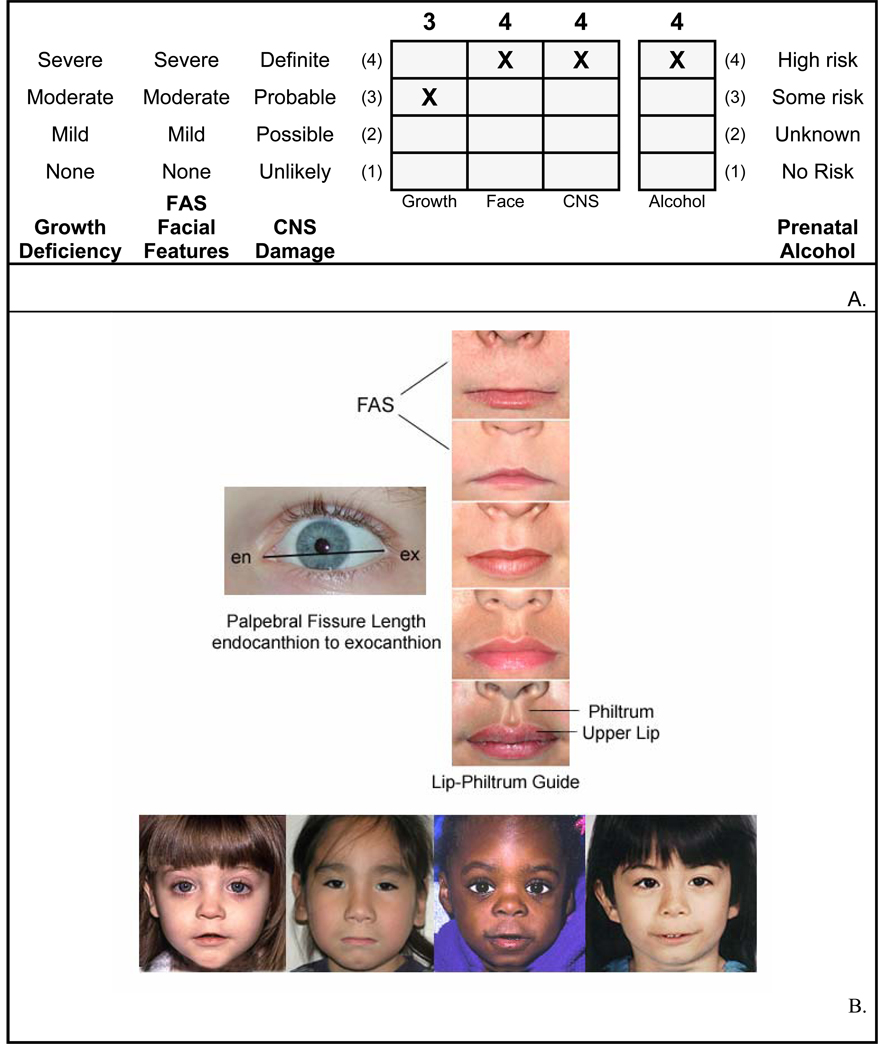
A comprehensive neuropsychological/psychiatric battery, coupled with MR imaging, (MRI), MR spectroscopy (MRS), and functional MRI (fMRI) assessments, were administered to children with fetal alcohol spectrum disorders (FASD) to determine if global and/or focal abnormalities could be identified, and distinguish diagnostic subclassifications across the spectrum. The 4 study groups included: (i) fetal alcohol syndrome (FAS)/partial FAS (PFAS); (ii) static encephalopathy/alcohol exposed (SE/AE); (iii) neurobehavioral disorder/alcohol exposed (ND/AE) as diagnosed with the FASD 4-Digit Code; and (iv) healthy peers with no prenatal alcohol exposure. Presented here are the MRI assessments that were used to compare the sizes of brain regions between the 4 groups. The neuropsychological/behavioral, MRS, and fMRI outcomes are reported separately.
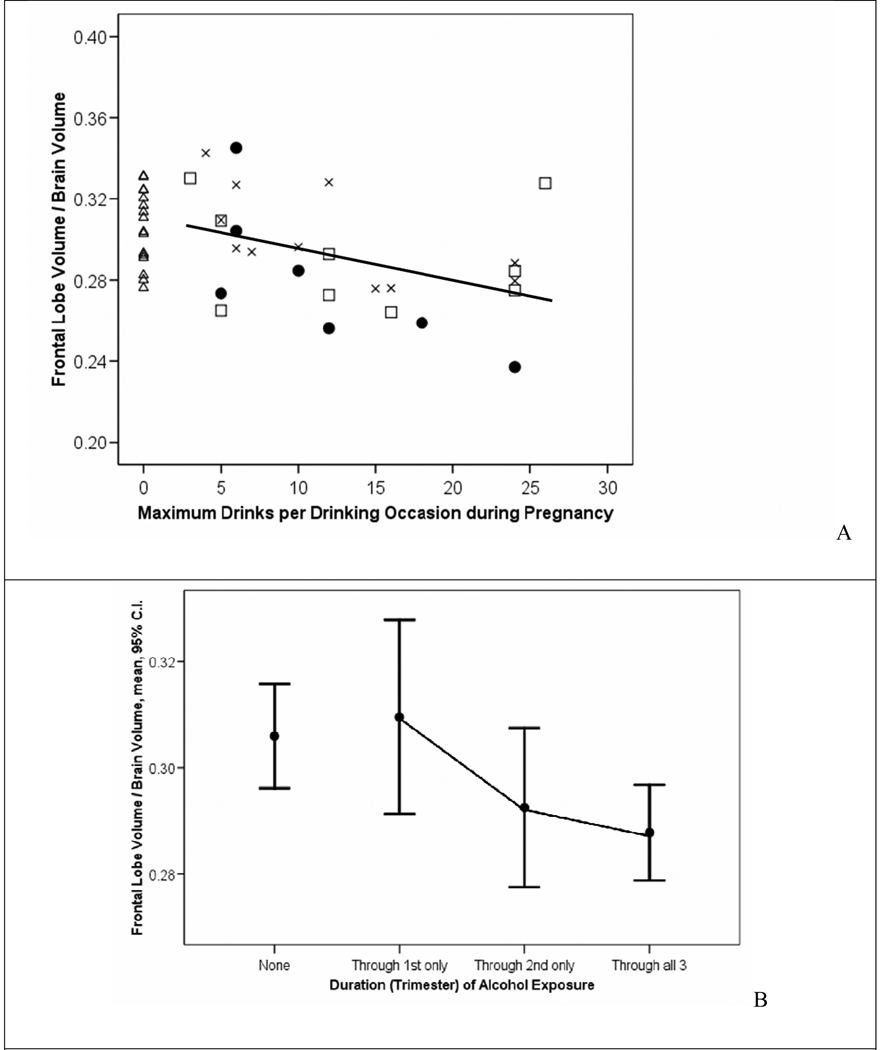
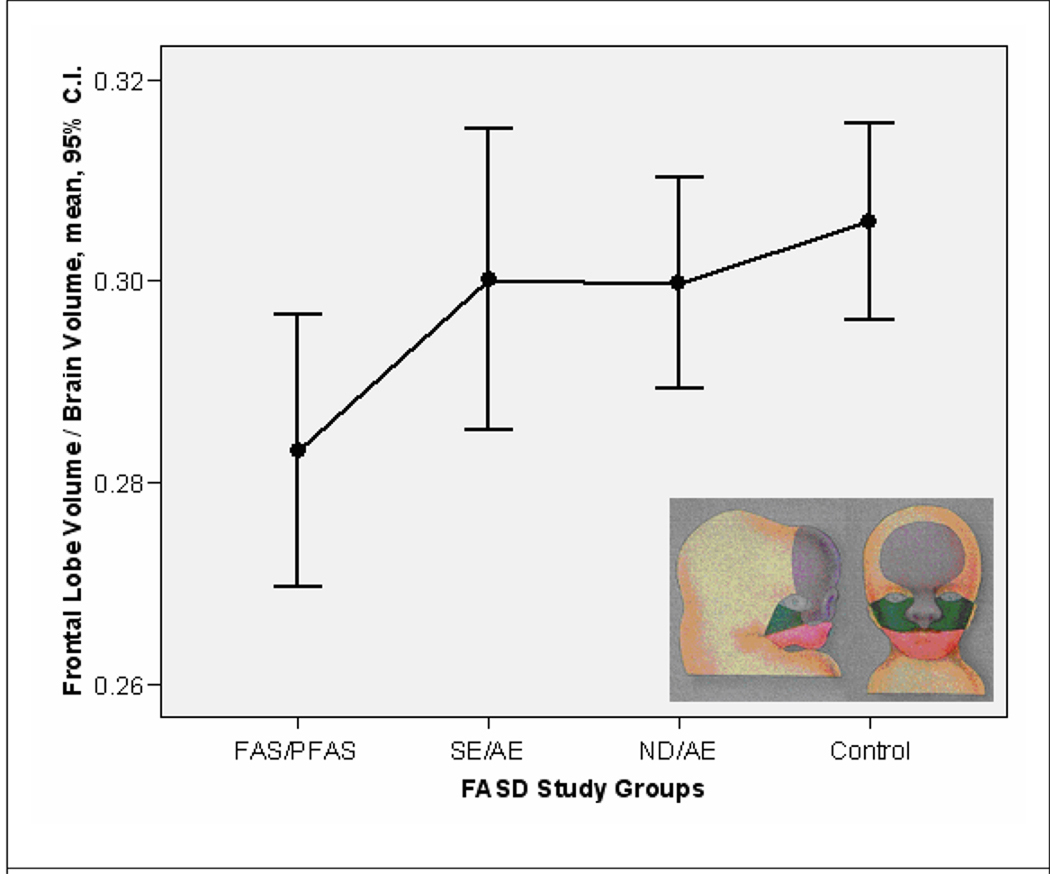
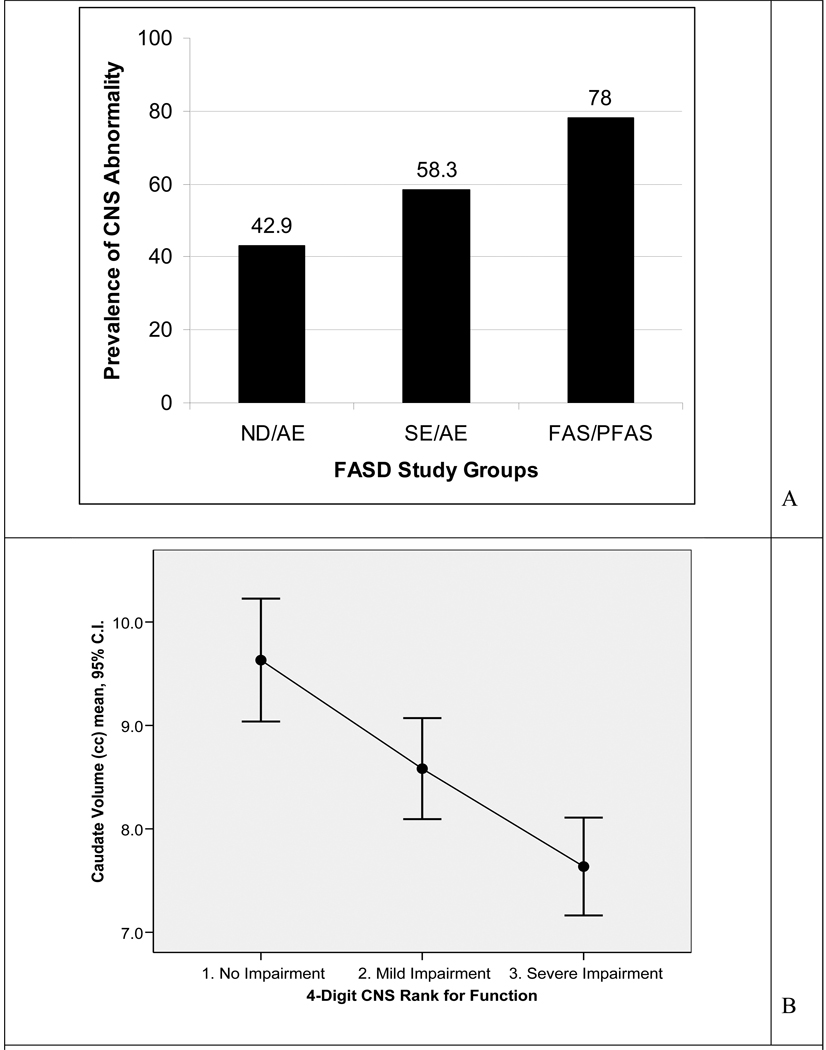
Progressing across the 4 study groups from Controls to ND/AE to SE/AE to FAS/PFAS, the mean absolute size of the total brain, frontal lobe, caudate, putamen, hippocampus, cerebellar vermis, and corpus callosum length decreased incrementally and significantly. The FAS/PFAS group (the only group with the 4-Digit FAS facial phenotype) had disproportionately smaller frontal lobes relative to all other groups. The FAS/PFAS and SE/AE groups [the 2 groups with the most severe central nervous system (CNS) dysfunction] had disproportionately smaller caudate regions relative to the ND/AE and Control groups. The prevalence of subjects in the FAS/PFAS, SE/AE, and ND/AE groups that had 1 or more brain regions, 2 or more SDs below the mean size observed in the Control group was 78, 58, and 43%, respectively. Significant correlations were observed between size of brain regions and level of prenatal alcohol exposure, magnitude of FAS facial phenotype, and level of CNS dysfunction.
Magnetic resonance imaging provided further validation that ND/AE, SE/AE, and FAS/PFAS as defined by the FASD 4-Digit Code are 3 clinically distinct and increasingly more affected diagnostic subclassifications under the umbrella of FASD. Neurostructural abnormalities are present across the spectrum. MRI could importantly augment diagnosis of conditions under the umbrella of FASD, once population-based norms for structural development of the human brain are established.
磁共振(MR)技术提供了用于评估神经异常的非侵入性方法。
对患有胎儿酒精谱系障碍(FASD)的儿童进行全面的神经心理学/精神病学测试、磁共振成像(MRI)、磁共振波谱(MRS)和功能性磁共振成像(fMRI)评估,以确定是否可以识别整体和/或局灶性异常,并区分谱内的诊断亚分类。这 4 个研究组包括:(i)胎儿酒精综合征(FAS)/部分 FAS(PFAS);(ii)静态脑病/酒精暴露(SE/AE);(iii)神经行为障碍/酒精暴露(ND/AE),根据 FASD 4 位数字代码诊断;(iv)无产前酒精暴露的健康同龄人。这里介绍的是用于比较 4 组之间脑区大小的 MRI 评估。神经心理学/行为、MRS 和 fMRI 结果分别报告。
在 4 个研究组中,从对照组到 ND/AE 到 SE/AE 再到 FAS/PFAS,大脑总容量、额叶、尾状核、壳核、海马体、小脑蚓部和胼胝体长度的平均绝对大小逐渐显著减小。FAS/PFAS 组(唯一具有 4 位数字 FAS 面部表型的组)的额叶相对所有其他组明显较小。FAS/PFAS 和 SE/AE 组(中枢神经系统(CNS)功能障碍最严重的 2 个组)的尾状核区域相对 ND/AE 和对照组明显较小。FAS/PFAS、SE/AE 和 ND/AE 组中,1 个或多个脑区大小低于对照组平均值 2 个标准差的受试者比例分别为 78%、58%和 43%。观察到大脑区域的大小与产前酒精暴露水平、FAS 面部表型的严重程度和中枢神经系统功能障碍的程度之间存在显著相关性。
磁共振成像进一步证实,根据 FASD 的 4 位数字代码定义的 ND/AE、SE/AE 和 FAS/PFAS 是 3 种临床上不同的、越来越受影响的诊断亚分类,它们都属于 FASD 这一保护伞下。整个谱中都存在神经结构异常。一旦建立了人类大脑结构发育的基于人群的正常标准,磁共振成像就可以重要地增强对 FASD 保护伞下疾病的诊断。