Diabetes Center, Federal University of São Paulo, São Paulo, Brazil.
Int J Clin Pract. 2009 Sep;63(9):1395-406. doi: 10.1111/j.1742-1241.2009.02143.x. Epub 2009 Jul 15.
Assess the efficacy and safety of saxagliptin added to a submaximal sulphonylurea dose vs. uptitration of sulphonylurea monotherapy in patients with type 2 diabetes and inadequate glycaemic control with sulphonylurea monotherapy.
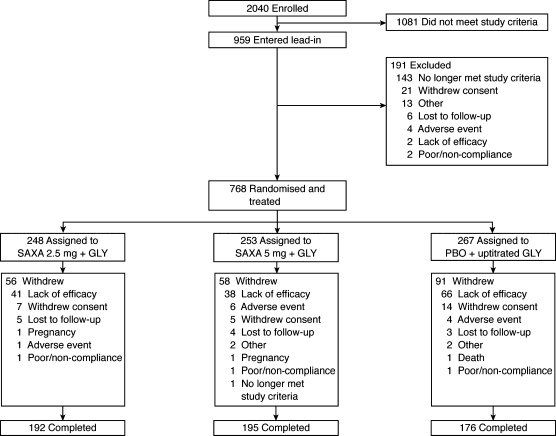
A total of 768 patients (18-77 years; HbA(1c) screening >or= 7.5 to <or= 10.0%) were randomised and treated with saxagliptin 2.5 or 5 mg in combination with glyburide 7.5 mg vs. glyburide 10 mg for 24 weeks. Blinded uptitration glyburide was allowed in the glyburide-only arm to a maximum total daily dose of 15 mg. Efficacy analyses were performed using ANCOVA and last-observation-carried-forward methodology.
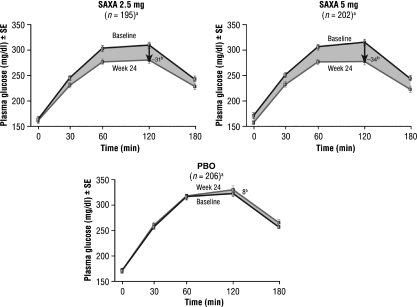
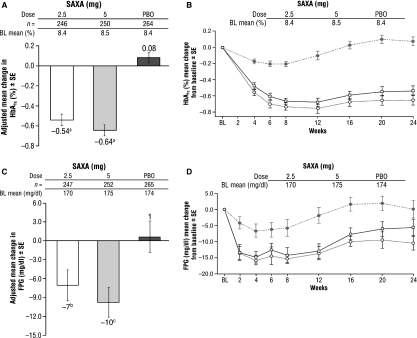
At week 24, 92% of glyburide-only patients were uptitrated to a total glyburide dose of 15 mg/day. Saxagliptin 2.5 and 5 mg provided statistically significant adjusted mean decreases from baseline to week 24 vs. uptitrated glyburide, respectively, in HbA(1c) (-0.54%, -0.64% vs. +0.08%; both p < 0.0001) and fasting plasma glucose (-7, -10 vs. +1 mg/dl; p = 0.0218 and p = 0.002). The proportion of patients achieving an HbA(1c) < 7% was greater for saxagliptin 2.5 and 5 mg vs. uptitrated glyburide (22.4% and 22.8% vs. 9.1%; both p < 0.0001). Postprandial glucose area under the curve was reduced for saxagliptin 2.5 and 5 mg vs. uptitrated glyburide (-4296 and -5000 vs. +1196 mg.min/dl; both p < 0.0001). Adverse event occurrence was similar across all groups. Reported hypoglycaemic events were not statistically significantly different for saxagliptin 2.5 (13.3%) and 5 mg (14.6%) vs. uptitrated glyburide (10.1%).
Saxagliptin added to submaximal glyburide therapy led to statistically significant improvements vs. uptitration of glyburide alone across key glycaemic parameters and was generally well tolerated.
评估在接受磺酰脲类药物单药治疗血糖控制不佳的 2 型糖尿病患者中,与磺酰脲类药物单药剂量递增相比,将沙格列汀加用至亚最大剂量磺酰脲类药物的疗效和安全性。
共纳入 768 例患者(18-77 岁;筛选时糖化血红蛋白(HbA1c)≥7.5%且<10.0%),这些患者被随机分为沙格列汀 2.5 或 5mg 联合格列吡嗪 7.5mg 组或格列吡嗪 10mg 组,接受为期 24 周的治疗。在格列吡嗪单药组中允许使用盲法将格列吡嗪逐渐加量至最大日总剂量 15mg。采用协方差分析和末次观察结转法进行疗效分析。
在第 24 周时,92%的格列吡嗪单药组患者的格列吡嗪剂量递增至 15mg/日的总剂量。与逐渐递增的格列吡嗪相比,沙格列汀 2.5 和 5mg 分别在第 24 周时提供了统计学上显著的 HbA1c(-0.54%,-0.64%vs.+0.08%;均p<0.0001)和空腹血糖(-7,-10 vs.+1mg/dl;p=0.0218 和 p=0.002)的调整平均降低。与逐渐递增的格列吡嗪相比,沙格列汀 2.5 和 5mg 使更多患者达到 HbA1c<7%(22.4%和 22.8%vs.9.1%;均p<0.0001)。沙格列汀 2.5 和 5mg 降低了餐后血糖曲线下面积(-4296 和-5000 vs.+1196mg.min/dl;均p<0.0001)。所有组的不良事件发生情况相似。沙格列汀 2.5(13.3%)和 5mg(14.6%)与逐渐递增的格列吡嗪(10.1%)相比,报告的低血糖事件发生率无统计学显著差异。
与单独逐渐递增格列吡嗪相比,沙格列汀联合亚最大剂量的格列吡嗪治疗可显著改善各项主要血糖参数,且通常具有良好的耐受性。