Sumaili Ernest K, Cohen Eric P, Zinga Chantal V, Krzesinski Jean-Marie, Pakasa Nestor M, Nseka Nazaire M
Nephrology Unit, University of Kinshasa, Kinshasa, Democratic Republic of Congo.
BMC Nephrol. 2009 Jul 21;10:18. doi: 10.1186/1471-2369-10-18.
There is limited knowledge of Chronic Kidney Disease (CKD) among high risk populations, especially in the developing countries. We report our study of testing for CKD in at-risk subjects.
In a cross-sectional study, 527 people from primary and secondary health care areas in the city of Kinshasa were studied from a random sample of at-risk out-patients with hypertension, diabetes, obesity, or HIV+. We measured blood pressure (BP), blood glucose level, proteinuria, body mass index, and estimated glomerular filtration rate (eGFR by MDRD equation) using calibrated creatinine levels based on one random measurement. The associations between health characteristics, indicators of kidney damage (proteinuria) and kidney function (<60 ml/min/1.73 m2) were also examined.
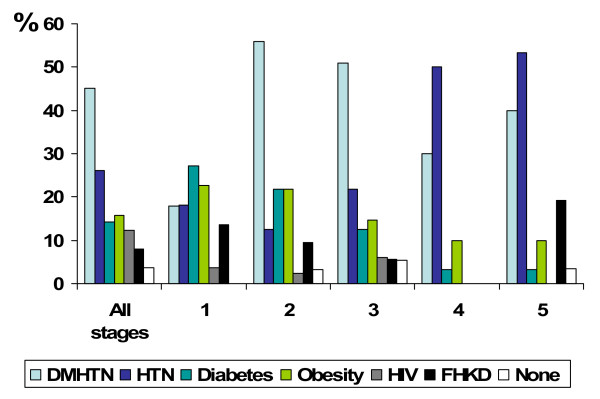
The prevalence of CKD in this study was 36%, but only 12% were aware of their condition. 4% of patients had stage 1 CKD, 6% stage 2, 18% stage 3, 2% stage 4, and 6% had stage 5. 24 hour quantitative proteinuria (>300 mg/day) was found in 19%. In those with the at-risk conditions, the % of CKD was: 44% in patients with hypertension, 39% in those with diabetes; 16% in the obese and 12% in those who were HIV+. 82% of those with a history of diabetes had elevated serum glucose levels at screening (>or= 126 mg/dl). Only 6% of individuals with hypertension having CKD had reduced BP to lower than 130/80 mmHg. In multivariate analysis, diabetes, proteinuria and hypertension were the strongest determinants of CKD 3+.
It appears that one out of three people in this at-risk population has undiagnosed CKD and poorly controlled CKD risk factors. This growing problem poses clear challenges to this developing country. Therefore, CKD should be addressed through the development of multidisciplinary teams and improved communication between traditional health care givers and nephrology services. Attention to CKD risk factors must become a priority.
高危人群,尤其是发展中国家的高危人群,对慢性肾脏病(CKD)的了解有限。我们报告了一项针对高危受试者进行CKD检测的研究。
在一项横断面研究中,从金沙萨市初级和二级卫生保健区域的527名高危门诊患者中随机抽取样本,这些患者患有高血压、糖尿病、肥胖症或HIV+。我们测量了血压(BP)、血糖水平、蛋白尿、体重指数,并根据一次随机测量的校准肌酐水平,使用MDRD方程估算肾小球滤过率(eGFR)。还研究了健康特征、肾脏损伤指标(蛋白尿)和肾功能(<60 ml/min/1.73 m2)之间的关联。
本研究中CKD的患病率为36%,但只有12%的人知晓自己的病情。4%的患者为1期CKD,6%为2期,18%为3期,2%为4期,6%为5期。19%的患者24小时定量蛋白尿(>300 mg/天)呈阳性。在患有高危疾病的患者中,CKD的患病率分别为:高血压患者中为44%,糖尿病患者中为39%;肥胖患者中为16%,HIV+患者中为12%。82%有糖尿病病史的患者在筛查时血糖水平升高(≥126 mg/dl)。患有CKD的高血压患者中只有6%的血压降至130/80 mmHg以下。在多变量分析中,糖尿病、蛋白尿和高血压是CKD 3+的最强决定因素。
在这一高危人群中,似乎三分之一的人患有未被诊断的CKD,且CKD危险因素控制不佳。这一日益严重的问题给这个发展中国家带来了严峻挑战。因此,应通过组建多学科团队以及改善传统医疗服务提供者与肾脏病服务之间的沟通来解决CKD问题。必须将关注CKD危险因素作为优先事项。