BMJ. 2009 Jul 28;339:b2546. doi: 10.1136/bmj.b2546.
To examine the effectiveness of cytological surveillance in primary care compared with immediate referral for colposcopic examination in women with low grade abnormal results on cervical cytology tests.
Multicentre individually randomised controlled trial.
NHS cervical screening programmes in Grampian, Tayside, and Nottingham.
4439 women, aged 20-59, with a cytology result showing borderline nuclear abnormalities or mild dyskaryosis, October 1999-October 2002.
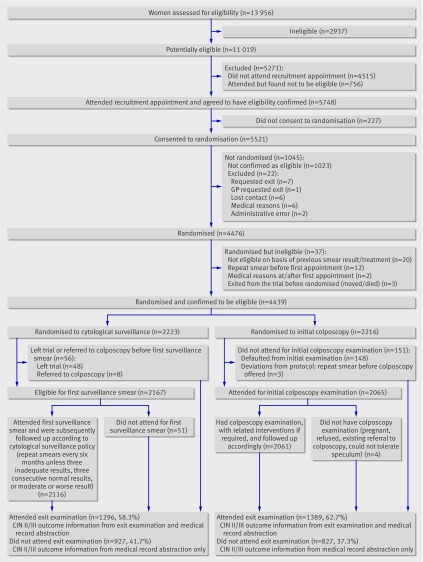
Cytological screening every six months in primary care (n=2223) or referral for colposcopy and related interventions (n=2216). All women were followed for three years, concluding with an exit appointment at which colposcopic examination was undertaken. Colposcopists assessing outcome at this appointment were blinded to randomisation.
Primary end point: cumulative incidence of cervical intraepithelial neoplasia grade II or more severe disease. Other end points: cervical intraepithelial neoplasia grade III or worse, clinically significant anxiety and depression, other self reported after effects, and rates of non-attendance. Analysis was by intention to treat; all those randomised were included.
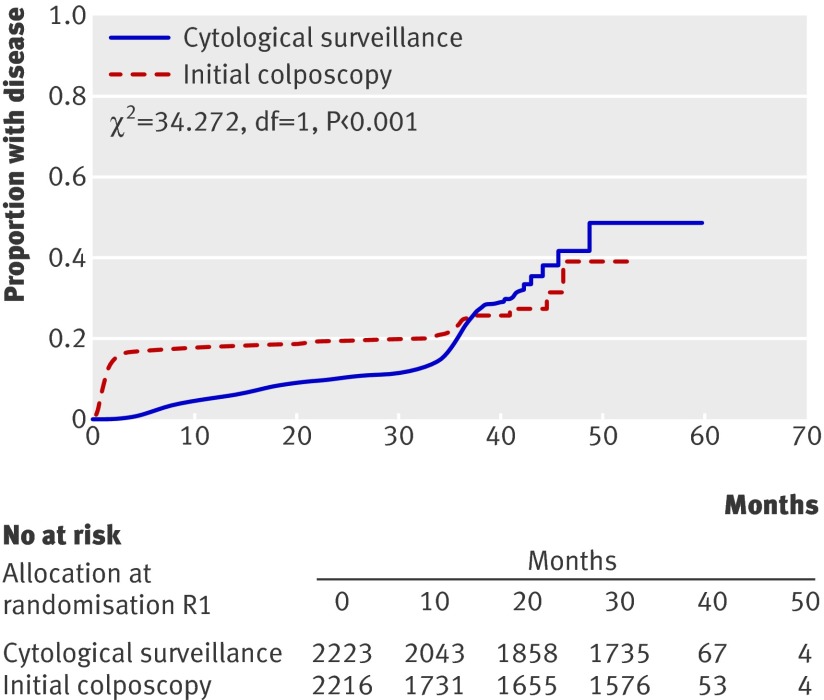
The cumulative incidence of cervical intraepithelial neoplasia grade II or worse was 79 per 1000 person years in the colposcopy arm and 58 per 1000 person years in the cytological surveillance arm (relative risk 1.37, 95% confidence interval 1.19 to 1.57). This difference was less marked for cervical intraepithelial neoplasia grade III or more severe disease, but the incidence was still higher in the colposcopy arm (relative risk 1.26, 1.04 to 1.53). Among women randomised to immediate colposcopy, 79% (74.9% to 82.5%) of cases of cervical intraepithelial neoplasia grade II or worse were diagnosed at the time of the immediate colposcopy, while among women randomised to cytological surveillance, 77% (72.1% to 81.2%) of cases were detected by surveillance cytology and related interventions. Similar proportions of women were anxious or depressed in the two arms. A higher proportion of women in the colposcopy arm reported after effects, and these were of longer duration and more severe. Non-attendance was low in both arms.
The more marked difference between the arms in the occurrence of cervical intraepithelial neoplasia grade II or worse than in the occurrence of grade III or worse can probably be accounted for by the spontaneous regression of some cases of grade II neoplasia. Compared with cytological surveillance, a policy of immediate colposcopy detects more cervical intraepithelial neoplasia grade II or worse, and some more grade III or worse, but might lead to overtreatment. Such a policy is associated with a higher rate of reported after effects, which are more severe and of longer duration than those associated with cytological surveillance.
ISRCTN 34841617.
比较在宫颈细胞学检查结果为低度异常的女性中,基层医疗中的细胞学监测与直接转诊进行阴道镜检查的有效性。
多中心个体随机对照试验。
格兰扁、泰赛德和诺丁汉的国民保健服务(NHS)宫颈筛查项目。
1999年10月至2002年10月期间,4439名年龄在20 - 59岁之间、细胞学结果显示核异常边界或轻度核异质的女性。
基层医疗中每六个月进行一次细胞学筛查(n = 2223)或转诊进行阴道镜检查及相关干预(n = 2216)。所有女性均随访三年,最后进行一次结束预约,届时进行阴道镜检查。评估此次预约结果的阴道镜检查医师对随机分组情况不知情。
主要终点:宫颈上皮内瘤变二级或更严重疾病的累积发病率。其他终点:宫颈上皮内瘤变三级或更差、具有临床意义的焦虑和抑郁、其他自我报告的后遗症以及未就诊率。分析采用意向性分析;所有随机分组的人都纳入分析。
阴道镜检查组宫颈上皮内瘤变二级或更差的累积发病率为每1000人年79例,细胞学监测组为每1000人年58例(相对风险1.37,95%置信区间1.19至1.57)。对于宫颈上皮内瘤变三级或更严重疾病,两组差异不太明显,但阴道镜检查组的发病率仍较高(相对风险1.26,1.04至1.53)。在随机分配接受直接阴道镜检查的女性中,79%(74.9%至82.5%)的宫颈上皮内瘤变二级或更差病例在直接阴道镜检查时被诊断出来,而在随机分配接受细胞学监测的女性中,77%(72.1%至81.2%)的病例通过监测细胞学检查及相关干预被检测出来。两组中焦虑或抑郁的女性比例相似。阴道镜检查组报告有后遗症的女性比例更高,且这些后遗症持续时间更长、更严重。两组的未就诊率都较低。
宫颈上皮内瘤变二级或更差的发生率在两组之间的差异比三级或更差的发生率差异更明显,这可能是由于一些二级瘤变病例的自发消退。与细胞学监测相比,直接阴道镜检查策略能检测出更多的宫颈上皮内瘤变二级或更差病例,以及一些更多的三级或更差病例,但可能导致过度治疗。这样的策略与报告的后遗症发生率较高相关,这些后遗症比与细胞学监测相关的后遗症更严重、持续时间更长。
ISRCTN 34841617