Malawi-Liverpool-Wellcome Trust Clinical Research Programme, Blantyre, Malawi.
PLoS One. 2009 Aug 13;4(8):e6621. doi: 10.1371/journal.pone.0006621.
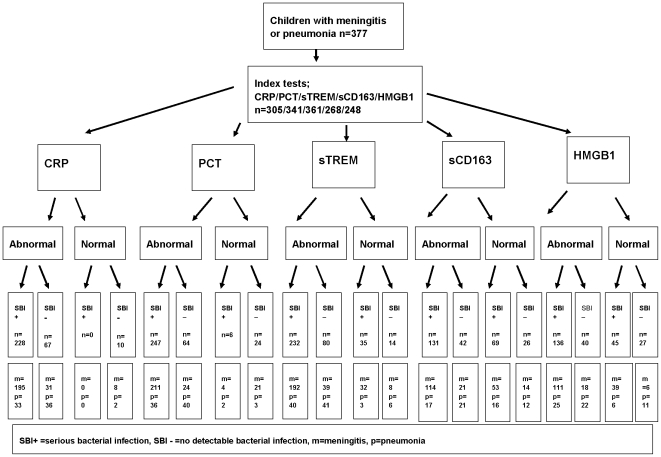
Early recognition and prompt and appropriate antibiotic treatment can significantly reduce mortality from serious bacterial infections (SBI). The aim of this study was to evaluate the utility of five markers of infection: C-reactive protein (CRP), procalcitonin (PCT), soluble triggering receptor expressed on myeloid cells-1 (sTREM-1), CD163 and high mobility group box-1 (HMGB1), as markers of SBI in severely ill Malawian children.
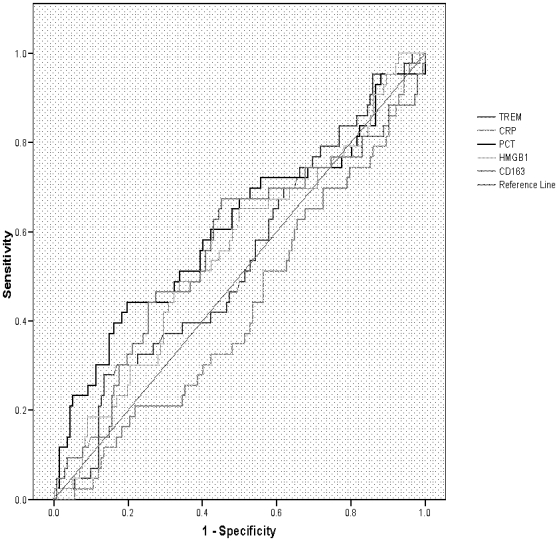
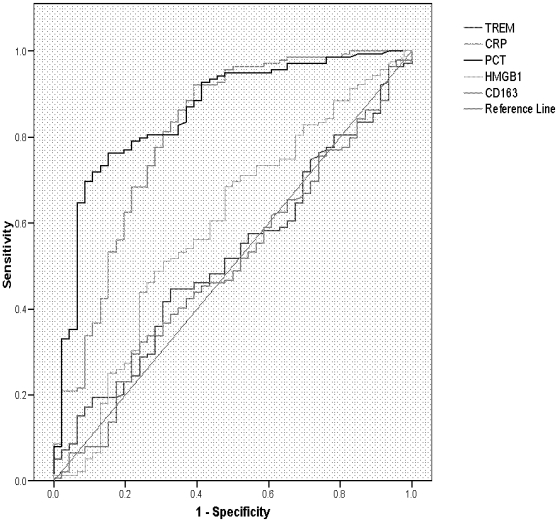
Children presenting with a signs of meningitis (n = 282) or pneumonia (n = 95), were prospectively recruited. Plasma samples were taken on admission for CRP, PCT, sTREM-1 CD163 and HMGB1 and the performance characteristics of each test to diagnose SBI and to predict mortality were determined. Of 377 children, 279 (74%) had SBI and 83 (22%) died. Plasma CRP, PCT, CD163 and HMGB1 and were higher in HIV-infected children than in HIV-uninfected children (p<0.01). In HIV-infected children, CRP and PCT were higher in children with SBI compared to those with no detectable bacterial infection (p<0.0005), and PCT and CD163 were higher in non-survivors (p = 0.001, p = 0.05 respectively). In HIV-uninfected children, CRP and PCT were also higher in children with SBI compared to those with no detectable bacterial infection (p<0.0005), and CD163 was higher in non-survivors (p = 0.05). The best predictors of SBI were CRP and PCT, and areas under the curve (AUCs) were 0.81 (95% CI 0.73-0.89) and 0.86 (95% CI 0.79-0.92) respectively. The best marker for predicting death was PCT, AUC 0.61 (95% CI 0.50-0.71).
Admission PCT and CRP are useful markers of invasive bacterial infection in severely ill African children. The study of these markers using rapid tests in a less selected cohort would be important in this setting.
早期识别和及时、恰当的抗生素治疗可以显著降低严重细菌感染(SBI)的死亡率。本研究旨在评估五种感染标志物:C 反应蛋白(CRP)、降钙素原(PCT)、髓系细胞触发受体-1 可溶性(sTREM-1)、CD163 和高迁移率族蛋白 1(HMGB1),作为马拉维重症儿童 SBI 的标志物。
前瞻性招募了出现脑膜炎(n = 282)或肺炎(n = 95)症状的儿童。入院时采集血浆样本用于 CRP、PCT、sTREM-1、CD163 和 HMGB1,并确定每种检测方法诊断 SBI 和预测死亡率的性能特征。在 377 名儿童中,279 名(74%)患有 SBI,83 名(22%)死亡。与未感染 HIV 的儿童相比,感染 HIV 的儿童的血浆 CRP、PCT、CD163 和 HMGB1 更高(p<0.01)。在感染 HIV 的儿童中,与无细菌感染的儿童相比,SBI 儿童的 CRP 和 PCT 更高(p<0.0005),非幸存者的 PCT 和 CD163 更高(p = 0.001,p = 0.05)。在未感染 HIV 的儿童中,与无细菌感染的儿童相比,SBI 儿童的 CRP 和 PCT 也更高(p<0.0005),非幸存者的 CD163 更高(p = 0.05)。SBI 的最佳预测因子是 CRP 和 PCT,曲线下面积(AUC)分别为 0.81(95%CI 0.73-0.89)和 0.86(95%CI 0.79-0.92)。预测死亡的最佳标志物是 PCT,AUC 为 0.61(95%CI 0.50-0.71)。
入院时的 PCT 和 CRP 是严重非洲儿童侵袭性细菌感染的有用标志物。在这种情况下,在选择较少的队列中使用快速检测研究这些标志物将非常重要。