Center for Policy and Research in Emergency Medicine, Department of Emergency Medicine, Oregon Health & Science University, 3181 SW Sam Jackson Park Road, Portland, OR 97239-3098, USA.
Ann Emerg Med. 2010 Mar;55(3):235-246.e4. doi: 10.1016/j.annemergmed.2009.07.024. Epub 2009 Sep 23.
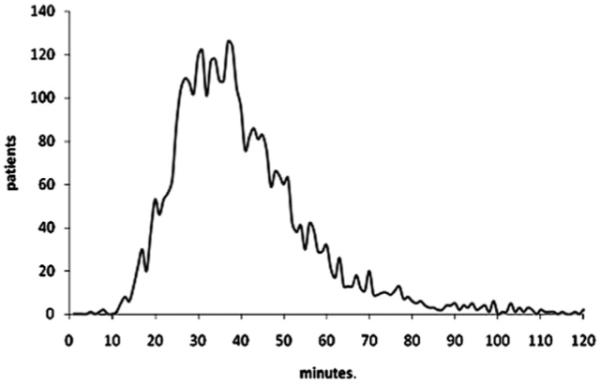
The first hour after the onset of out-of-hospital traumatic injury is referred to as the "golden hour," yet the relationship between time and outcome remains unclear. We evaluate the association between emergency medical services (EMS) intervals and mortality among trauma patients with field-based physiologic abnormality.
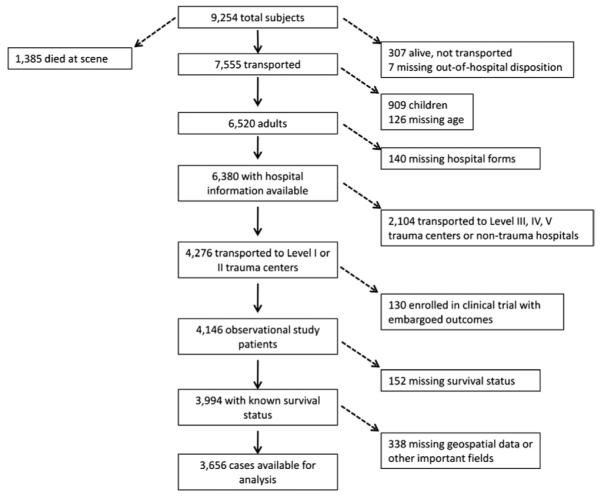
This was a secondary analysis of an out-of-hospital, prospective cohort registry of adult (aged > or =15 years) trauma patients transported by 146 EMS agencies to 51 Level I and II trauma hospitals in 10 sites across North America from December 1, 2005, through March 31, 2007. Inclusion criteria were systolic blood pressure less than or equal to 90 mm Hg, respiratory rate less than 10 or greater than 29 breaths/min, Glasgow Coma Scale score less than or equal to 12, or advanced airway intervention. The outcome was in-hospital mortality. We evaluated EMS intervals (activation, response, on-scene, transport, and total time) with logistic regression and 2-step instrumental variable models, adjusted for field-based confounders.
There were 3,656 trauma patients available for analysis, of whom 806 (22.0%) died. In multivariable analyses, there was no significant association between time and mortality for any EMS interval: activation (odds ratio [OR] 1.00; 95% confidence interval [CI] 0.95 to 1.05), response (OR 1.00; 95% CI 9.97 to 1.04), on-scene (OR 1.00; 95% CI 0.99 to 1.01), transport (OR 1.00; 95% CI 0.98 to 1.01), or total EMS time (OR 1.00; 95% CI 0.99 to 1.01). Subgroup and instrumental variable analyses did not qualitatively change these findings.
In this North American sample, there was no association between EMS intervals and mortality among injured patients with physiologic abnormality in the field.
院外创伤性损伤发生后的第一个小时被称为“黄金时间”,但时间与结局之间的关系尚不清楚。我们评估了现场生理异常的创伤患者的紧急医疗服务(EMS)时间间隔与死亡率之间的关系。
这是对 2005 年 12 月 1 日至 2007 年 3 月 31 日期间北美 10 个地点的 146 个 EMS 机构向 51 个 I 级和 II 级创伤医院转运的成人(年龄≥15 岁)创伤患者的院外前瞻性队列登记处的二次分析。纳入标准为收缩压≤90mmHg,呼吸频率<10 次/分或>29 次/分,格拉斯哥昏迷评分≤12 分或需要高级气道干预。结局为院内死亡率。我们使用逻辑回归和两步工具变量模型评估 EMS 时间间隔(激活、反应、现场、转运和总时间),并根据现场混杂因素进行调整。
共有 3656 例创伤患者可用于分析,其中 806 例(22.0%)死亡。多变量分析中,任何 EMS 时间间隔与死亡率之间均无显著关联:激活(比值比[OR]1.00;95%置信区间[CI]0.95 至 1.05)、反应(OR 1.00;95% CI 9.97 至 1.04)、现场(OR 1.00;95% CI 0.99 至 1.01)、转运(OR 1.00;95% CI 0.98 至 1.01)或总 EMS 时间(OR 1.00;95% CI 0.99 至 1.01)。亚组和工具变量分析并未改变这些发现的性质。
在这个北美样本中,现场存在生理异常的创伤患者的 EMS 时间间隔与死亡率之间没有关联。