Avidan Michael S, Searleman Adam C, Storandt Martha, Barnett Kara, Vannucci Andrea, Saager Leif, Xiong Chengjie, Grant Elizabeth A, Kaiser Dagmar, Morris John C, Evers Alex S
Cardiothoracic Anesthesiology and Cardiothoracic Intensive Care, Department of Anesthesiology, Washington University in St. Louis, Missouri 63110-1093, USA.
Anesthesiology. 2009 Nov;111(5):964-70. doi: 10.1097/ALN.0b013e3181bc9719.
Persistent postoperative cognitive decline is thought to be a public health problem, but its severity may have been overestimated because of limitations in statistical methodology. This study assessed whether long-term cognitive decline occurred after surgery or illness by using an innovative approach and including participants with early Alzheimer disease to overcome some limitations.
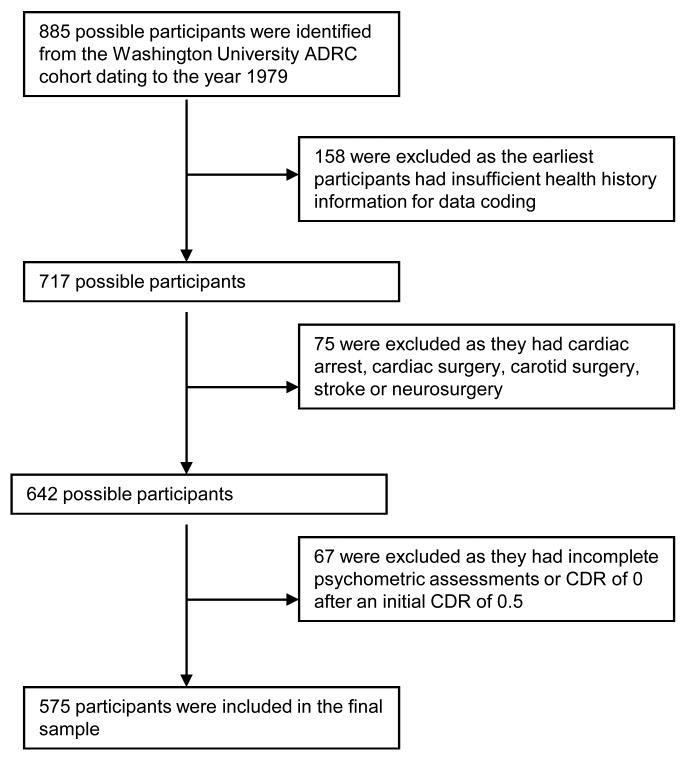
In this retrospective cohort study, three groups were identified from participants tested annually at the Washington University Alzheimer's Disease Research Center in St. Louis, Missouri: those with noncardiac surgery, illness, or neither. This enabled long-term tracking of cognitive function before and after surgery and illness. The effect of surgery and illness on longitudinal cognitive course was analyzed using a general linear mixed effects model. For participants without initial dementia, time to dementia onset was analyzed using sequential Cox proportional hazards regression.
Of the 575 participants, 214 were nondemented and 361 had very mild or mild dementia at enrollment. Cognitive trajectories did not differ among the three groups (surgery, illness, control), although demented participants declined more markedly than nondemented participants. Of the initially nondemented participants, 23% progressed to a clinical dementia rating greater than zero, but this was not more common after surgery or illness.
The study did not detect long-term cognitive decline independently attributable to surgery or illness, nor were these events associated with accelerated progression to dementia. The decision to proceed with surgery in elderly people, including those with early Alzheimer disease, may be made without factoring in the specter of persistent cognitive deterioration.
术后持续性认知功能下降被认为是一个公共卫生问题,但其严重程度可能因统计方法的局限性而被高估。本研究采用一种创新方法并纳入早期阿尔茨海默病患者以克服一些局限性,评估手术后或患病后是否会出现长期认知功能下降。
在这项回顾性队列研究中,从密苏里州圣路易斯华盛顿大学阿尔茨海默病研究中心每年接受测试的参与者中确定了三组:接受非心脏手术的患者、患病患者或两者皆无的患者。这使得能够对手术和患病前后的认知功能进行长期跟踪。使用一般线性混合效应模型分析手术和疾病对纵向认知过程的影响。对于最初没有痴呆的参与者,使用序贯Cox比例风险回归分析痴呆发病时间。
575名参与者中,214名在入组时无痴呆,361名有非常轻度或轻度痴呆。三组(手术、疾病、对照)的认知轨迹没有差异,尽管痴呆患者的下降比非痴呆患者更明显。在最初无痴呆的参与者中,23%进展到临床痴呆评分为零以上,但这在手术或患病后并不更常见。
该研究未发现手术或疾病独立导致的长期认知功能下降,这些事件也与痴呆进展加速无关。在决定对老年人,包括早期阿尔茨海默病患者进行手术时,可能无需考虑持续性认知恶化的因素。