Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
J Appl Clin Med Phys. 2009 Oct 7;10(4):132-141. doi: 10.1120/jacmp.v10i4.2982.
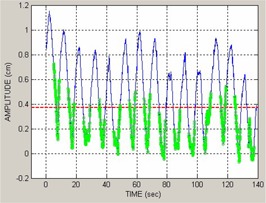
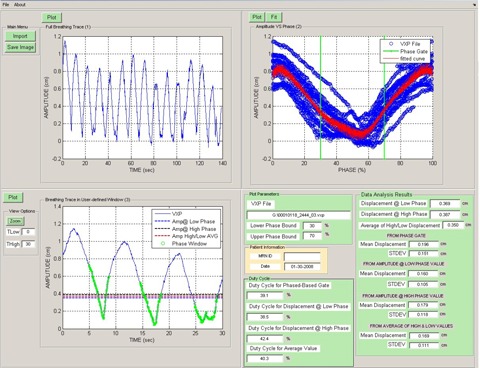
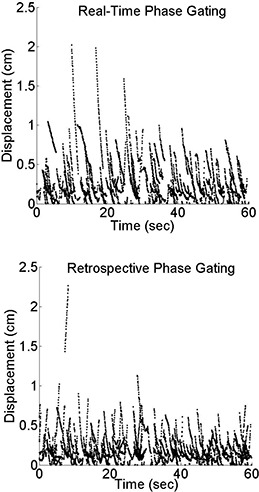
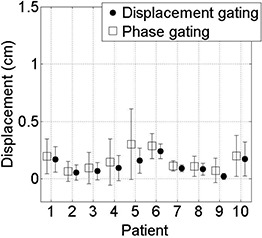
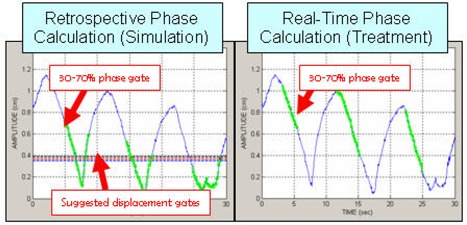
The Varian Real-time Position Management (RPM) system allows respiratory gating based on either the phase or displacement (amplitude) of the breathing waveform. A problem in clinical application is that phase-based gating, required for respiration-correlated (4D-CT) simulation, is not robust to irregular breathing patterns during treatment, and a widely used system version (1.6) does not provide an easy means to change from a phase-based gate into an equivalent displacement-based one. We report on the development and evaluation of a robust method to convert phase-gate thresholds, set by the physician, into equivalent displacement-gate thresholds to facilitate its clinical application to treatment. The software tool analyzes the respiration trace recorded during the 4D-CT simulation, and determines a relationship between displacement and phase through a functional fit. The displacement gate thresholds are determined from an average of two values of this function, corresponding to the start and end thresholds of the original phase gate. The software tool was evaluated in two ways: first, whether in-gate residual target motion and predicted treatment beam duty cycle are equivalent between displacement gating and phase gating during 4D-CT simulation (using retrospective phase recalculation); second, whether residual motion is improved with displacement gating during treatment relative to phase gating (using real-time phase calculation). Residual target motion was inferred from the respiration traces and quantified in terms of mean and standard deviation in-gate displacement measured relative to the value at the start of the recorded trace. For retrospectively-calculated breathing traces compared with real-time calculated breathing traces, we evaluate the inaccuracies of real-time phase calculation by measuring the phase gate position in each trace as well as the mean in-gate displacement and standard deviation of the displacement. Retrospectively-calculated data from ten patients were analyzed. The patient averaged in-gate mean +/- standard deviation displacement (representing residual motion) was reduced from 0.16 +/- 0.14 cm for phase gating under simulation conditions to 0.12 +/- 0.08 cm for displacement gating. Evaluation of respiration traces under treatment conditions (real-time phase calculation) showed that the average displacement gate threshold results in a lower in-gate mean and residual motion (variance) for all patients studied. The patient-averaged in-gate mean +/- standard deviation displacement was reduced from 0.26 +/- 0.18 cm for phase gating (under treatment conditions) to 0.15 +/- 0.09 cm for displacement gating. Real-time phase gating sometimes leads to gating on incorrect portions of the breathing cycle when the breathing trace is irregular. Displacement gating is less prone to such errors, as evidenced by the lower in-gate residual motion in a large majority of cases.
瓦里安实时位置管理(RPM)系统允许基于呼吸波形的相位或位移(幅度)进行呼吸门控。临床应用中的一个问题是,相位门控用于与呼吸相关的(4D-CT)模拟,但在治疗期间对不规则的呼吸模式不稳定,并且广泛使用的系统版本(1.6)没有提供一种简单的方法将相位门控转换为等效的位移门控。我们报告了一种稳健的方法的开发和评估,该方法将医生设定的相位门控阈值转换为等效的位移门控阈值,以促进其在治疗中的临床应用。该软件工具分析在 4D-CT 模拟期间记录的呼吸轨迹,并通过功能拟合确定位移和相位之间的关系。通过该函数的两个值的平均值确定位移门控阈值,这两个值对应于原始相位门控的起始和结束阈值。该软件工具通过两种方式进行了评估:首先,在 4D-CT 模拟期间,位移门控和相位门控之间的门内残留目标运动和预测的治疗射束占空比是否等效(使用回顾性相位重新计算);其次,与相位门控相比,治疗期间残留运动是否通过位移门控得到改善(使用实时相位计算)。残留目标运动是从呼吸轨迹中推断出来的,并根据相对于记录轨迹起始时的值测量的门内位移的平均值和标准偏差来量化。对于与实时计算的呼吸轨迹相比的回顾性计算的呼吸轨迹,我们通过测量每个轨迹中的相位门控位置以及位移的门内位移平均值和标准偏差来评估实时相位计算的不准确性。分析了十个患者的回顾性计算数据。在模拟条件下,相位门控的患者平均门内位移(代表残留运动)从 0.16 ± 0.14cm 减少到 0.12 ± 0.08cm 用于位移门控。在治疗条件下(实时相位计算)评估呼吸轨迹表明,对于所有研究的患者,平均位移门控阈值导致门内平均位移和残留运动(方差)降低。相位门控(在治疗条件下)的患者平均门内位移为 0.26 ± 0.18cm,位移门控的患者平均门内位移为 0.15 ± 0.09cm。当呼吸轨迹不规则时,实时相位门控有时会导致在呼吸周期的不正确部分进行门控。位移门控不太容易出现此类错误,这从大多数情况下较低的门内残留运动中可以看出。