Department of Radiation Oncology, RWTH Aachen University Hospital, Pauwelsstrasse 30, 52074 Aachen Germany.
Radiat Oncol. 2009 Nov 23;4:57. doi: 10.1186/1748-717X-4-57.
Biological brain tumor imaging using O-(2-[18F]fluoroethyl)-L-tyrosine (FET)-PET combined with inverse treatment planning for locally restricted dose escalation in patients with glioblastoma multiforme seems to be a promising approach.The aim of this study was to compare inverse with forward treatment planning for an integrated boost dose application in patients suffering from a glioblastoma multiforme, while biological target volumes are based on FET-PET and MRI data sets.
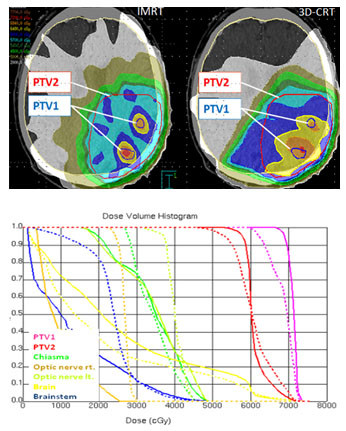
In 16 glioblastoma patients an intensity-modulated radiotherapy technique comprising an integrated boost (IB-IMRT) and a 3-dimensional conventional radiotherapy (3D-CRT) technique were generated for dosimetric comparison. FET-PET, MRI and treatment planning CT (P-CT) were co-registrated. The integrated boost volume (PTV1) was auto-contoured using a cut-off tumor-to-brain ratio (TBR) of > or = 1.6 from FET-PET. PTV2 delineation was MRI-based. The total dose was prescribed to 72 and 60 Gy for PTV1 and PTV2, using daily fractions of 2.4 and 2 Gy.
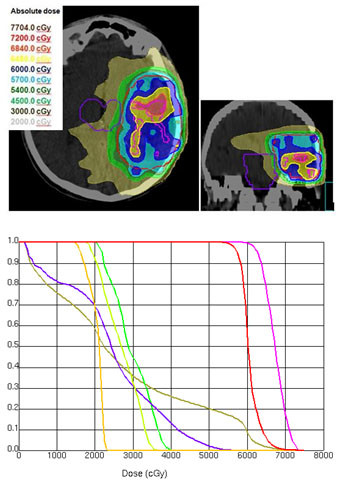
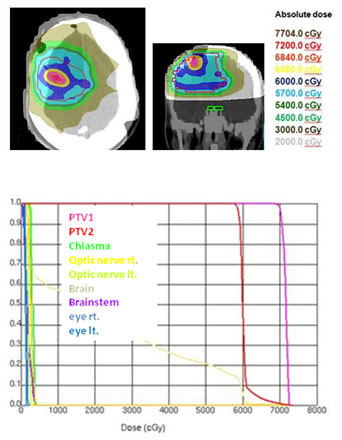
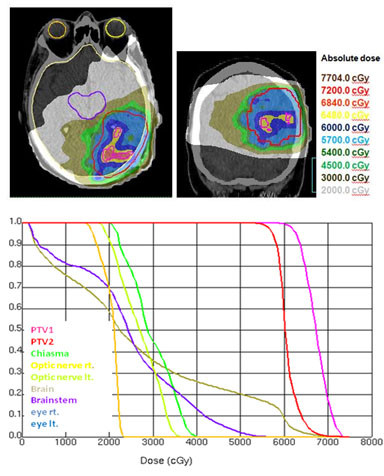
After auto-contouring of PTV1 a marked target shape complexity had an impact on the dosimetric outcome. Patients with 3-4 PTV1 subvolumes vs. a single volume revealed a significant decrease in mean dose (67.7 vs. 70.6 Gy). From convex to complex shaped PTV1 mean doses decreased from 71.3 Gy to 67.7 Gy. The homogeneity and conformity for PTV1 and PTV2 was significantly improved with IB-IMRT. With the use of IB-IMRT the minimum dose within PTV1 (61.1 vs. 57.4 Gy) and PTV2 (51.4 vs. 40.9 Gy) increased significantly, and the mean EUD for PTV2 was improved (59.9 vs. 55.3 Gy, p < 0.01). The EUD for PTV1 was only slightly improved (68.3 vs. 67.3 Gy). The EUD for the brain was equal with both planning techniques.
In the presented planning study the integrated boost concept based on inversely planned IB-IMRT is feasible. The FET-PET-based automatically contoured PTV1 can lead to very complex geometric configurations, limiting the achievable mean dose in the boost volume. With IB-IMRT a better homogeneity and conformity, compared to 3D-CRT, could be achieved.
使用 O-(2-[18F] 氟乙基)-L-酪氨酸 (FET)-PET 进行生物脑肿瘤成像,并结合反向治疗计划,以在多形性胶质母细胞瘤患者中进行局部受限的剂量升级,这似乎是一种很有前途的方法。本研究的目的是比较在患有多形性胶质母细胞瘤的患者中应用基于 FET-PET 和 MRI 数据集的综合增强剂量的反向与正向治疗计划,同时基于生物靶区体积。
在 16 名多形性胶质母细胞瘤患者中,生成了强度调制放疗技术,包括综合增强 (IB-IMRT) 和三维常规放疗 (3D-CRT) 技术,以进行剂量比较。FET-PET、MRI 和治疗计划 CT(P-CT)进行了配准。使用 FET-PET 的肿瘤与脑比值(TBR)>或=1.6 的截断值自动勾画综合增强体积(PTV1)。PTV2 的勾画基于 MRI。PTV1 和 PTV2 的总剂量分别规定为 72 和 60 Gy,使用 2.4 和 2 Gy 的每日分次剂量。
PTV1 自动勾画后,明显的靶区形状复杂性对剂量结果有影响。与单个 PTV1 亚体积相比,具有 3-4 个 PTV1 亚体积的患者平均剂量明显降低(67.7 与 70.6 Gy)。从凸形到复杂形状的 PTV1 平均剂量从 71.3 Gy 降至 67.7 Gy。PTV1 和 PTV2 的均匀性和适形性均显著提高,与 IB-IMRT 相比。使用 IB-IMRT,PTV1(61.1 与 57.4 Gy)和 PTV2(51.4 与 40.9 Gy)的最小剂量显著增加,并且 PTV2 的平均 EUD 得到改善(59.9 与 55.3 Gy,p<0.01)。PTV1 的 EUD 仅略有改善(68.3 与 67.3 Gy)。脑的 EUD 与两种计划技术相同。
在本研究中,基于反演计划的 IB-IMRT 的综合增强概念是可行的。基于 FET-PET 的自动勾画的 PTV1 可能导致非常复杂的几何形状,限制了增强体积中的可实现平均剂量。与 3D-CRT 相比,IB-IMRT 可以实现更好的均匀性和适形性。