Division of General Internal Medicine, Brigham and Women's Hospital, 1620 Tremont Street, 3rd Floor, Boston, MA 02120-1613, USA.
J Gen Intern Med. 2010 Mar;25(3):211-9. doi: 10.1007/s11606-009-1196-1. Epub 2009 Dec 15.
Previous studies of hospital readmission have focused on specific conditions or populations and generated complex prediction models.
To identify predictors of early hospital readmission in a diverse patient population and derive and validate a simple model for identifying patients at high readmission risk.
Prospective observational cohort study.
Participants encompassed 10,946 patients discharged home from general medicine services at six academic medical centers and were randomly divided into derivation (n = 7,287) and validation (n = 3,659) cohorts.
We identified readmissions from administrative data and 30-day post-discharge telephone follow-up. Patient-level factors were grouped into four categories: sociodemographic factors, social support, health condition, and healthcare utilization. We performed logistic regression analysis to identify significant predictors of unplanned readmission within 30 days of discharge and developed a scoring system for estimating readmission risk.
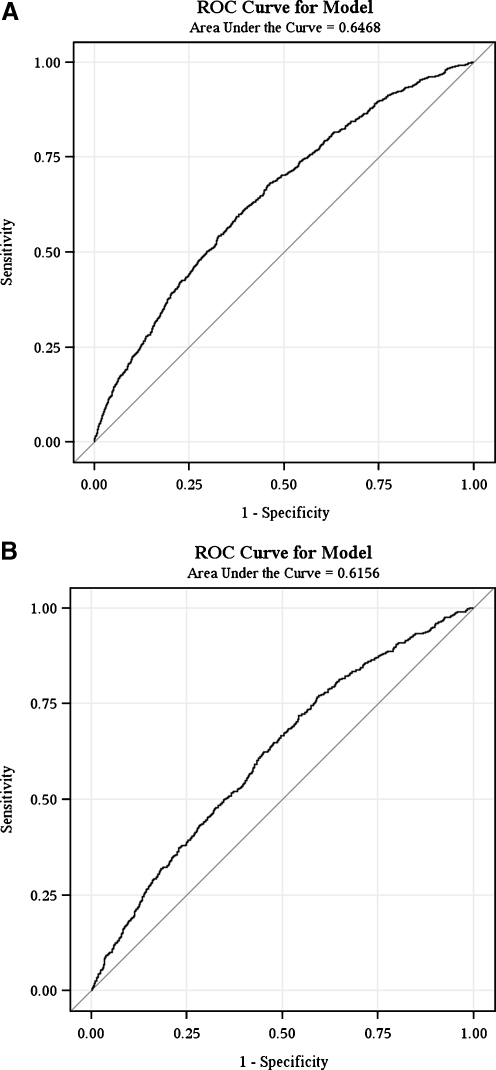
Approximately 17.5% of patients were readmitted in each cohort. Among patients in the derivation cohort, seven factors emerged as significant predictors of early readmission: insurance status, marital status, having a regular physician, Charlson comorbidity index, SF12 physical component score, >or=1 admission(s) within the last year, and current length of stay >2 days. A cumulative risk score of >or=25 points identified 5% of patients with a readmission risk of approximately 30% in each cohort. Model discrimination was fair with a c-statistic of 0.65 and 0.61 for the derivation and validation cohorts, respectively.
Select patient characteristics easily available shortly after admission can be used to identify a subset of patients at elevated risk of early readmission. This information may guide the efficient use of interventions to prevent readmission.
先前关于医院再入院的研究集中于特定的情况或人群,并生成了复杂的预测模型。
确定来自不同患者群体的早期医院再入院的预测因素,并制定和验证一种简单的模型,以识别高再入院风险的患者。
前瞻性观察性队列研究。
参与者包括来自六个学术医疗中心的一般医学服务出院回家的 10946 名患者,随机分为推导(n=7287)和验证(n=3659)队列。
我们从行政数据和出院后 30 天的电话随访中确定再入院情况。患者水平的因素分为四类:社会人口因素、社会支持、健康状况和医疗保健利用。我们进行逻辑回归分析以确定出院后 30 天内无计划再入院的显著预测因素,并制定了一个估计再入院风险的评分系统。
在每个队列中,大约 17.5%的患者再入院。在推导队列的患者中,有七个因素成为早期再入院的显著预测因素:保险状况、婚姻状况、有固定医生、Charlson 合并症指数、SF12 生理成分评分、过去一年中>或=1 次入院和当前住院时间>2 天。>或=25 分的累积风险评分确定了每个队列中 5%的患者再入院风险约为 30%。模型的区分度为中等,推导和验证队列的 c 统计量分别为 0.65 和 0.61。
入院后不久就可以获得的一些患者特征可以用于识别具有早期再入院风险升高的患者亚组。这些信息可能有助于指导有效利用干预措施预防再入院。