Department of Ophthalmology, The Mount Sinai School of Medicine, New York, New York, USA.
Ophthalmology. 2010 Mar;117(3):576-84. doi: 10.1016/j.ophtha.2009.08.010. Epub 2010 Jan 19.
To evaluate the clinical outcomes of cyclosporine treatment for noninfectious ocular inflammation.
Retrospective cohort study.
A total of 373 patients with noninfectious ocular inflammation managed at 4 tertiary ocular inflammation clinics in the United States observed to use cyclosporine as a single noncorticosteroid immunosuppressive agent to their treatment regimen, between 1979 and 2007 inclusive.
Participants were identified from the Systemic Immunosuppressive Therapy for Eye Diseases Cohort Study. Demographic and clinical characteristics, including dosage of cyclosporine and main outcome measures, were obtained for every eye of every patient at every visit via medical record review by trained expert reviewers.
Control of inflammation, sustained control after reducing corticosteroid dosages, and discontinuation of therapy because of toxicity.
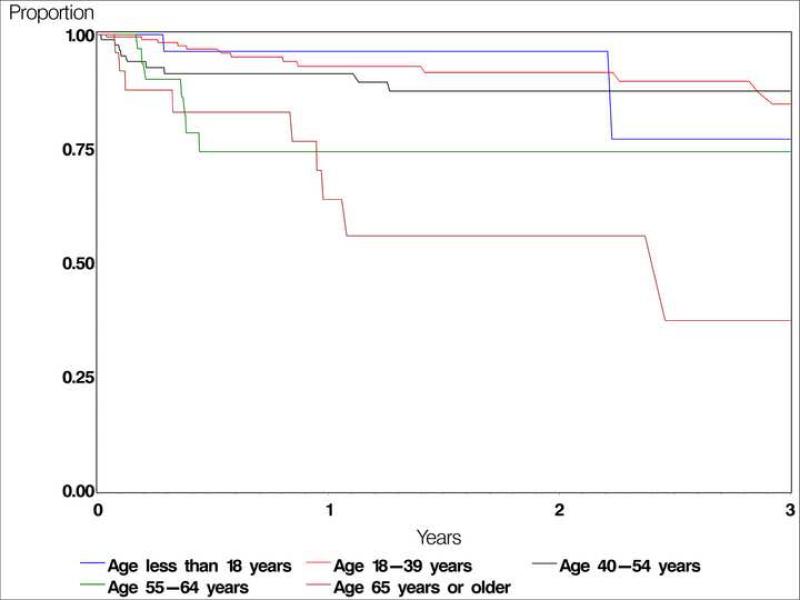
Of the 373 patients (681 eyes) initiating cyclosporine monotherapy, 33.4% by 6 months and 51.9% by 1 year gained sustained, complete control of inflammation over at least 2 visits spanning at least 28 days. Approximately 25% more improved to a level of slight inflammatory activity by each of these time points. Corticosteroid-sparing success (completely controlled inflammation for at least 28 days with prednisone < or = 10 mg/day) was achieved by 22.1% by 6 months and 36.1% within 1 year. Toxicity led to discontinuation of therapy within 1 year by 10.7% of the population. Patients aged more than 55 years were more than 3-fold more likely to discontinue therapy because of toxicity than patients aged 18 to 39 years. Doses of 151 to 250 mg/day tended to be more successful than lower doses and were not associated with a higher discontinuation for toxicity rate; higher doses did not seem to offer a therapeutic advantage.
Cyclosporine, with corticosteroid therapy as indicated, was modestly effective for controlling ocular inflammation. Our data support a preference for cyclosporine adult dosing between 151 and 250 mg/day. Although cyclosporine was tolerated by the majority of patients, toxicity was more frequent with increasing age; alternative agents may be preferred for patients aged more than 55 years.
评估环孢素治疗非感染性眼部炎症的临床疗效。
回顾性队列研究。
1979 年至 2007 年间,美国 4 家三级眼部炎症诊所共 373 例非感染性眼部炎症患者接受环孢素单药治疗作为唯一的非皮质类固醇免疫抑制剂,纳入本研究。
通过系统免疫抑制治疗眼部疾病队列研究确定参与者。通过培训的专家审查者对每位患者每只眼的每次就诊的病历进行回顾,获取人口统计学和临床特征,包括环孢素剂量和主要观察指标。
炎症控制、减少皮质类固醇剂量后的持续控制以及因毒性而停止治疗。
在开始环孢素单药治疗的 373 例患者(681 只眼)中,33.4%在 6 个月时和 51.9%在 1 年时获得至少 2 次就诊至少 28 天的持续完全炎症控制。到这些时间点,约有 25%的患者改善到轻度炎症活动程度。在 6 个月和 1 年内,分别有 22.1%和 36.1%的患者达到皮质类固醇节约成功(泼尼松剂量≤10mg/d,至少 28 天完全控制炎症)。10.7%的患者在 1 年内因毒性而停止治疗。年龄大于 55 岁的患者因毒性而停止治疗的可能性是年龄 18 至 39 岁患者的 3 倍以上。151 至 250mg/d 剂量组比低剂量组更有效,且与更高的毒性停药率无关;高剂量似乎没有提供治疗优势。
环孢素与皮质类固醇治疗联合应用,对控制眼部炎症有一定疗效。我们的数据支持环孢素成人剂量在 151 至 250mg/d 之间的选择。尽管大多数患者耐受环孢素,但毒性随年龄增长而增加;对于年龄大于 55 岁的患者,可能需要选择替代药物。