Department of Neurology, University Hospital of Muenster, Muenster, Germany.
Diabetes Care. 2010 Mar;33(3):639-44. doi: 10.2337/dc09-1740. Epub 2009 Dec 23.
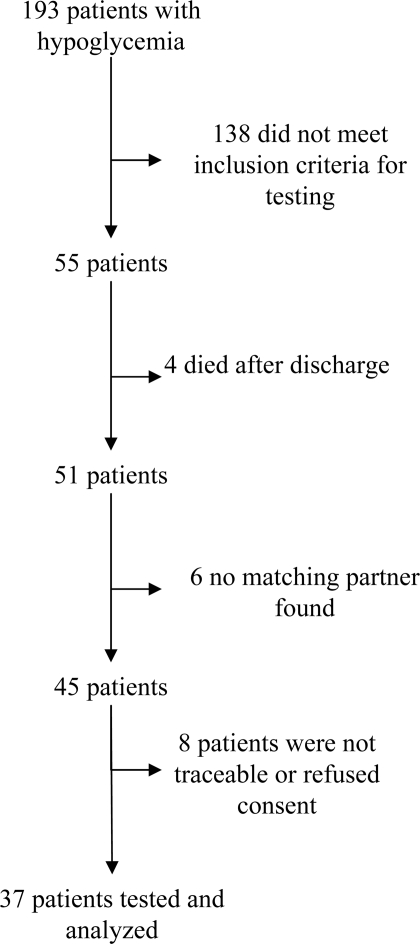
OBJECTIVE Tight glycemic control (TGC) in critically ill patients is associated with an increased risk of hypoglycemia. Whether those short episodes of hypoglycemia are associated with adverse morbidity and mortality is a matter of discussion. Using a case-control study design, we investigated whether hypoglycemia under TGC causes permanent neurocognitive dysfunction in patients surviving critical illness. RESEARCH DESIGN AND METHODS From our patient data management system, we identified adult survivors treated for >72 h in our surgical intensive care unit (ICU) between 2004 and 2007 (n = 4,635) without a history of neurocognitive dysfunction or structural brain abnormalities who experienced at least one episode of hypoglycemia during treatment (hypo group) (n = 37). For each hypo group patient, one patient stringently matched for demographic- and disease-related data were identified as a control subject. We performed a battery of neuropsychological tests investigating five areas of cognitive functioning in both groups at least 1 year after ICU discharge. Test results were compared with data from healthy control subjects and between groups. RESULTS Critical illness caused neurocognitive dysfunction in all tested domains in both groups. The dysfunction was aggravated in hypo group patients in one domain, namely that of visuospatial skills (P < 0.01). Besides hypoglycemia, both hyperglycemia (r = -0.322; P = 0.005) and fluctuations of blood glucose (r = -0.309; P = 0.008) were associated with worse test results in this domain. CONCLUSIONS Hypoglycemia was found to aggravate critical illness-induced neurocognitive dysfunction to a limited, but significant, extent; however, an impact of hyperglycemia and fluctuations of blood glucose on neurocognitive function cannot be excluded.
危重病患者的严格血糖控制(TGC)与低血糖风险增加有关。这些短暂的低血糖发作是否与不良发病率和死亡率有关,这是一个讨论的问题。使用病例对照研究设计,我们研究了在危重病存活患者中,TGC 下的低血糖是否会导致永久性神经认知功能障碍。
我们从患者数据管理系统中确定了 2004 年至 2007 年期间在我们外科重症监护病房(ICU)接受>72 小时治疗且无神经认知功能障碍或结构性脑异常史的成年幸存者(n=4635),并在治疗期间经历了至少一次低血糖发作(低血糖组)(n=37)。对于每组低血糖组患者,均严格匹配一名在人口统计学和疾病相关数据方面匹配的患者作为对照。我们对两组患者在 ICU 出院后至少 1 年进行了一系列神经心理学测试,以评估五个认知功能领域。比较两组的测试结果与健康对照组的数据,并进行组间比较。
危重病在两组所有测试领域均导致神经认知功能障碍。在一个领域,即视觉空间技能领域,低血糖组患者的功能障碍更为严重(P<0.01)。除低血糖外,高血糖(r=-0.322;P=0.005)和血糖波动(r=-0.309;P=0.008)均与该领域的测试结果较差相关。
发现低血糖会在有限但显著的程度上加重危重病引起的神经认知功能障碍;然而,不能排除高血糖和血糖波动对神经认知功能的影响。