Department of Neurosurgery, University of Maryland School of Medicine, Baltimore, Maryland 21201-1595, USA.
J Neurosurg. 2010 Sep;113(3):622-9. doi: 10.3171/2009.11.JNS081052.
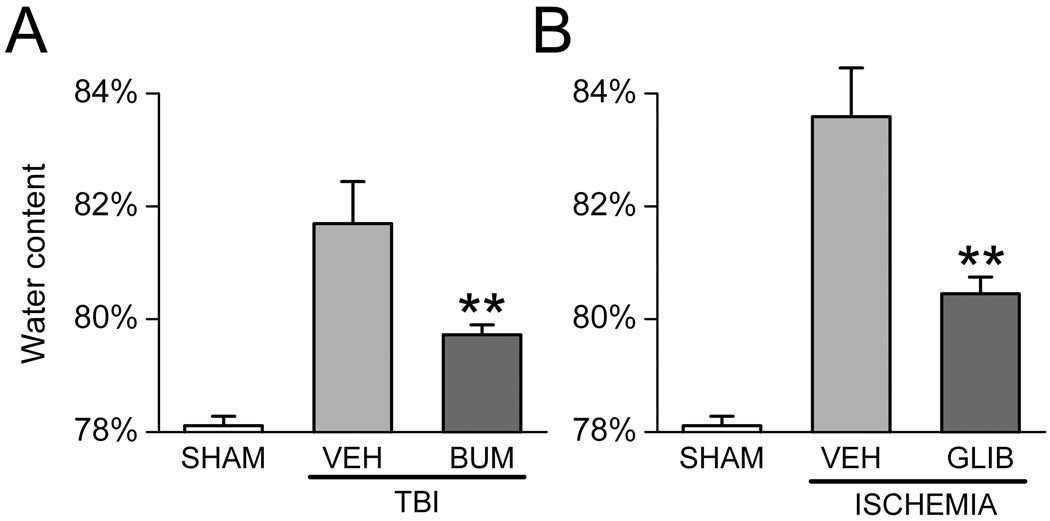
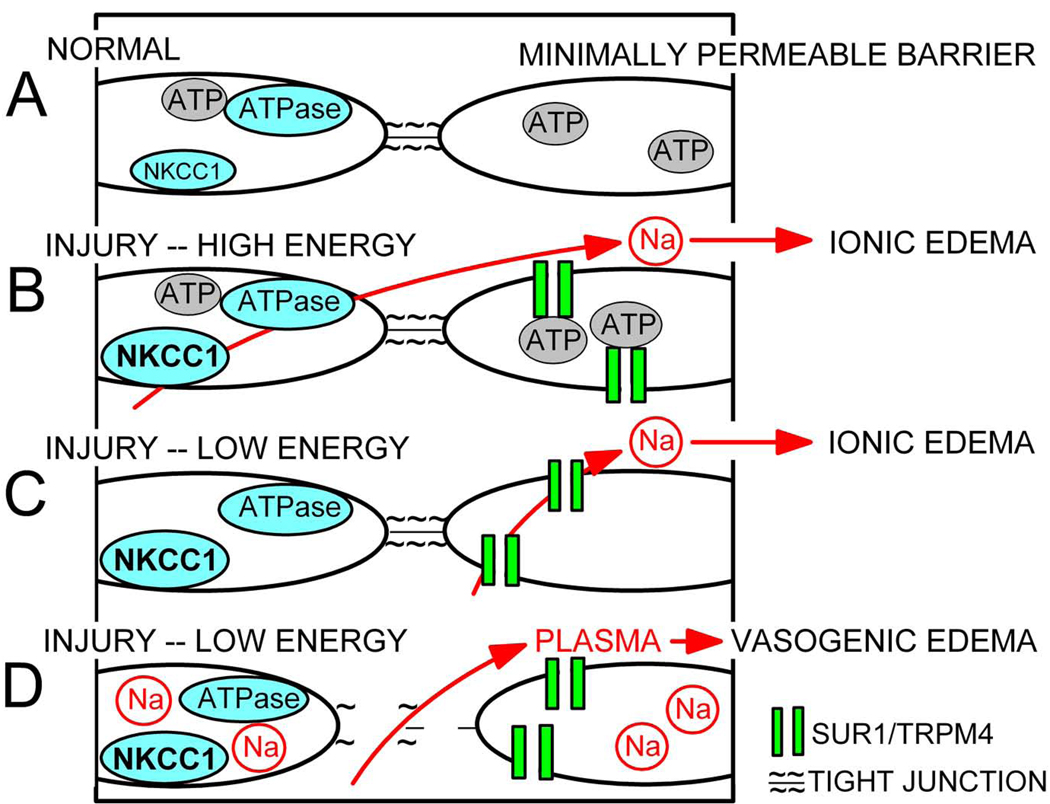
Microvascular failure largely underlies the damaging secondary events that accompany traumatic brain injury (TBI). Changes in capillary permeability result in the extravasation of extracellular fluid, inflammatory cells, and blood, thereby producing cerebral edema, inflammation, and progressive secondary hemorrhage (PSH). Recent work in rat models of TBI and stroke have implicated 2 ion transport proteins expressed in brain endothelial cells as critical mediators of edema formation: the constitutively expressed Na(+)-K(+)-2Cl(-) cotransporter, NKCC1, and the trauma/ischemia-induced SUR1-regulated NC(Ca-ATP) (SUR1/TRPM4) channel. Whereas NKCC1 function requires adenosine 5'-triphosphate (ATP), activation of SUR1/TRPM4 occurs only after ATP depletion. This opposite dependence on intracellular ATP levels implies that one or the other mechanism will activate/deactivate as ATP concentrations rise and fall during periods of ischemia/reperfusion, resulting in continuous edema formation regardless of cellular energy status. Moreover, with critical ATP depletion, sustained opening of SUR1/TRPM4 channels results in the oncotic death of endothelial cells, leading to capillary fragmentation and PSH. Bumetanide and glibenclamide are 2 well-characterized, safe, FDA-approved drugs that inhibit NKCC1 and the SUR1/TRPM4 channel, respectively. When used alone, these drugs have provided documented beneficial effects in animal models of TBI- and ischemiaassociated cerebral edema and PSH. Given the mechanistic and temporal differences by which NKCC1 and the SUR1/TRPM4 channel contribute to the pathophysiological mechanisms of these events, combination therapy with bumetanide and glibenclamide may yield critical synergy in preventing injury-associated capillary failure.
微血管衰竭在创伤性脑损伤 (TBI) 伴随的破坏性继发性事件中起着重要作用。毛细血管通透性的变化导致细胞外液、炎症细胞和血液的渗出,从而产生脑水肿、炎症和进行性继发性出血 (PSH)。最近在 TBI 和中风的大鼠模型中的研究表明,在脑内皮细胞中表达的 2 种离子转运蛋白是水肿形成的关键介质:持续表达的 Na(+)-K(+)-2Cl(-)共转运蛋白 NKCC1 和创伤/缺血诱导的 SUR1 调节的 NC(Ca-ATP) (SUR1/TRPM4) 通道。虽然 NKCC1 的功能需要三磷酸腺苷 (ATP),但 SUR1/TRPM4 的激活仅在 ATP 耗尽后发生。这种对细胞内 ATP 水平的相反依赖性意味着,在缺血/再灌注期间,随着细胞内 ATP 浓度的升高和降低,一种或另一种机制将激活/失活,导致持续的水肿形成,而与细胞能量状态无关。此外,随着关键的 ATP 耗竭,SUR1/TRPM4 通道的持续开放导致内皮细胞的渗透死亡,导致毛细血管碎裂和 PSH。布美他尼和格列本脲是两种经过充分研究的、安全的、获得美国食品和药物管理局批准的药物,分别抑制 NKCC1 和 SUR1/TRPM4 通道。当单独使用时,这些药物在 TBI 和与缺血相关的脑水肿和 PSH 的动物模型中提供了有文件证明的有益效果。鉴于 NKCC1 和 SUR1/TRPM4 通道对这些事件的病理生理机制的贡献的机制和时间差异,布美他尼和格列本脲的联合治疗可能在预防与损伤相关的毛细血管衰竭方面产生关键的协同作用。