Institute of Tropical Medicine, Antwerp, Belgium.
Malar J. 2010 Jan 20;9:23. doi: 10.1186/1475-2875-9-23.
Despite Vietnam's success in reducing malaria mortality and morbidity over the last decade, malaria persists in the forested and mountainous areas of the central and southern provinces, where more than 50% of the clinical cases and 90% of severe cases and malaria deaths occur.
Between July 2005 and September 2006, a multi-method study, triangulating a malariometric cross-sectional survey and qualitative data from focused ethnography, was carried out among the Ra-glai ethnic minority in the hilly forested areas of south-central Vietnam.
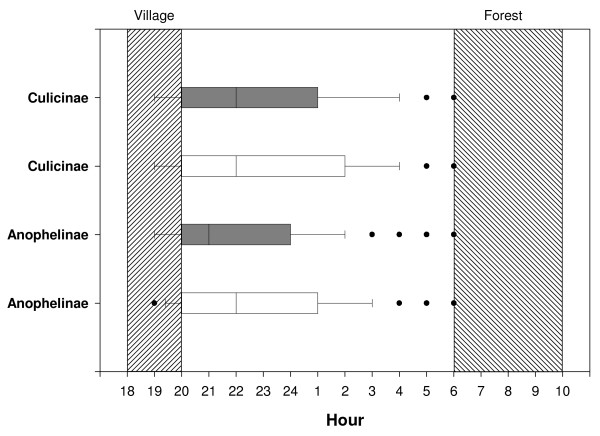
Despite the relatively high malaria burden among the Ra-glai and their general awareness that mosquitoes can transmit an unspecific kind of fever (84.2%), the use of bed nets, distributed free of charge by the national malaria control programme, remains low at the farmers' forest fields where the malaria risk is the highest. However, to meet work requirements during the labour intensive malaria transmission and rainy season, Ra-glai farmers combine living in government supported villages along the road with a second home or shelter at their slash and burn fields located in the forest. Bed net use was 84.6% in the villages but only 52.9% at the forest fields; 20.6% of the respondents slept unprotected in both places. Such low use may be explained by the low perception of the risk for malaria, decreasing the perceived need to sleep protected. Several reasons may account for this: (1) only 15.6% acknowledged the higher risk of contracting malaria in the forest than in the village; (2) perceived mosquito biting times only partially coincided with Anopheles dirus ss and Anopheles minimus A true biting times; (3) the disease locally identified as 'malaria' was hardly perceived as having an impact on forest farmers' daily lives as they were unaware of the specific kind of fevers from which they had suffered even after being diagnosed with malaria at the health centre (20.9%).
The progressive confinement of malaria to minority groups and settings in the Greater Mekong sub-region implies that further success in malaria control will be linked to research into these specific socio-cultural contexts. Findings highlight the need for context sensitive malaria control policies; not only to reduce the local malaria burden but also to minimize the risk of malaria spreading to other areas where transmission has virtually ceased.
尽管越南在过去十年中成功降低了疟疾的死亡率和发病率,但在中南部的森林和山区,疟疾仍然存在,那里超过 50%的临床病例、90%的重症病例和疟疾死亡病例发生。
2005 年 7 月至 2006 年 9 月,在越南北部中南部丘陵森林地区的拉莱少数民族中,采用了一种多方法研究,将疟疾计量横断面调查和来自重点民族志的定性数据相结合。
尽管拉莱人疟疾负担相对较高,并且他们普遍意识到蚊子可以传播一种非特异性的发热(84.2%),但国家疟疾控制规划免费分发的蚊帐在疟疾风险最高的农民森林田地的使用仍然很低。然而,为了满足劳动密集型疟疾传播和雨季的工作要求,拉莱农民在道路旁的政府支持的村庄生活,同时在森林中的烧荒田地拥有第二个家或避难所。在村庄里,蚊帐的使用率为 84.6%,而在森林里只有 52.9%;20.6%的受访者在这两个地方都没有保护措施地睡觉。这种低使用率可能是由于对疟疾风险的认识较低,从而降低了对受保护睡眠的需求。有几个原因可以解释这一点:(1)只有 15.6%的人承认在森林中感染疟疾的风险高于在村庄中;(2)蚊子叮咬时间的感知与按蚊 s 和微小按蚊的真正叮咬时间只有部分重合;(3)当地被确定为“疟疾”的疾病几乎没有被认为对森林农民的日常生活有影响,因为他们不知道自己所患的具体发热类型,甚至在卫生中心被诊断为疟疾后(20.9%)。
大湄公河次区域的疟疾逐渐局限于少数民族和特定环境,这意味着进一步成功控制疟疾将与对这些特定社会文化背景的研究相关。研究结果强调需要制定针对具体情况的疟疾控制政策;不仅要降低当地疟疾负担,还要最大限度地减少疟疾传播到其他几乎已经停止传播的地区的风险。