University of Edinburgh, Royal Infirmary of Edinburgh, UK.
Br J Cancer. 2010 Feb 16;102(4):665-72. doi: 10.1038/sj.bjc.6605532. Epub 2010 Jan 26.
Macrophage inhibitory cytokine-1(MIC-1) is a potential modulator of systemic inflammation and nutritional depletion, both of which are adverse prognostic factors in oesophago-gastric cancer (OGC).
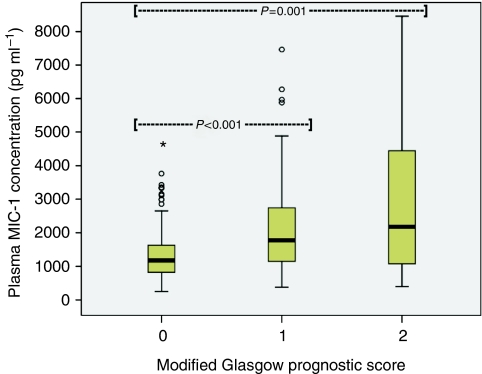
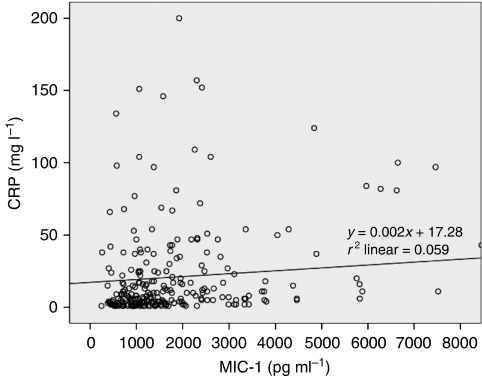
Plasma MIC-1, systemic inflammation (defined as plasma C-reactive protein (CRP) of > or =10 mg l(-1) or modified Glasgow prognostic score (mGPS) of > or =1), and nutritional status were assessed in newly diagnosed OGC patients (n=293). Healthy volunteers (n=35) served as controls.
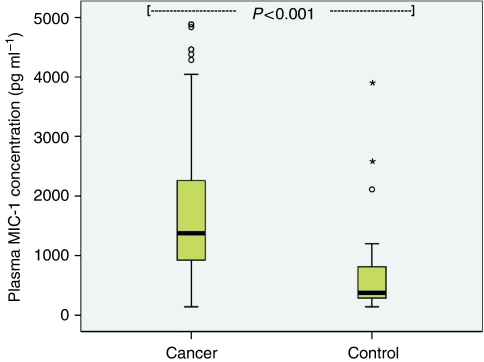
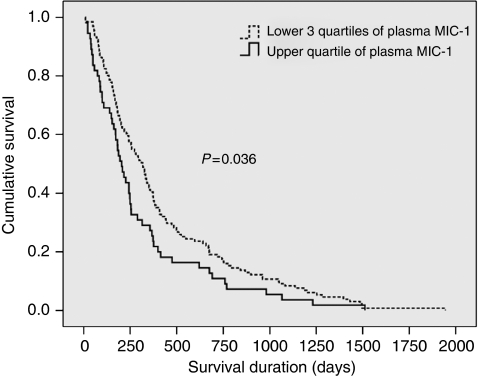
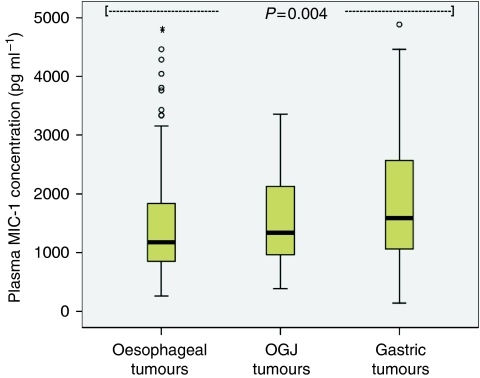
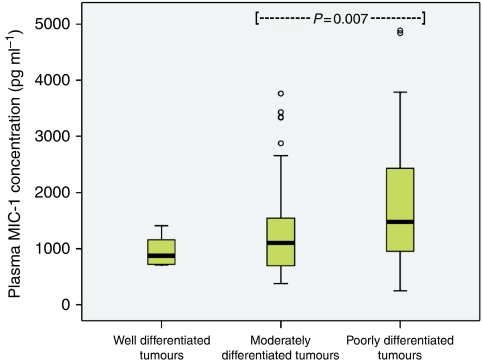
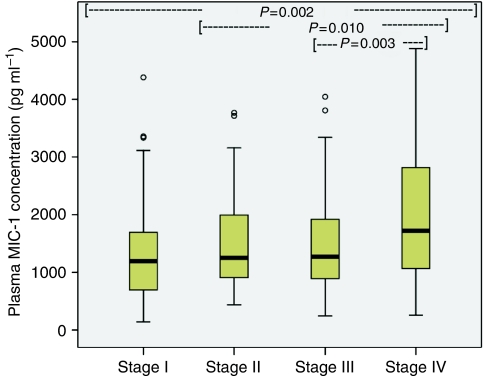
MIC-1 was elevated in patients (median=1371 pg ml(-1); range 141-39 053) when compared with controls (median=377 pg ml(-1); range 141-3786; P<0.001). Patients with gastric tumours (median=1592 pg ml(-1); range 141-12 643) showed higher MIC-1 concentrations than patients with junctional (median=1337 pg ml(-1); range 383-39 053) and oesophageal tumours (median=1180 pg ml(-1); range 258-31 184; P=0.015). Patients showed a median weight loss of 6.4% (range 0.0-33.4%), and 42% of patients had an mGPS of > or =1 or plasma CRP of > or =10 mg l(-1) (median=9 mg l(-1); range 1-200). MIC-1 correlated positively with disease stage (r(2)=0.217; P<0.001), age (r(2)=0.332; P<0.001), CRP (r(2)=0.314; P<0.001), and mGPS (r(2)=0.336; P<0.001), and negatively with Karnofsky Performance Score (r(2)=-0.269; P<0.001). However, although MIC-1 correlated weakly with dietary intake (r(2)=0.157; P=0.031), it did not correlate with weight loss, BMI, or anthropometry. Patients with MIC-1 levels in the upper quartile showed reduced survival (median=204 days; 95% CI 157-251) when compared with patients with MIC-1 levels in the lower three quartiles (median=316 days; 95% CI 259-373; P=0.036), but MIC-1 was not an independent prognostic indicator.
There is no independent link between plasma MIC-1 levels and depleted nutritional status or survival in OGC.
巨噬细胞抑制因子-1(MIC-1)是一种潜在的全身炎症和营养耗竭的调节剂,而全身炎症和营养耗竭是胃癌(OGC)的不良预后因素。
对 293 例新诊断的 OGC 患者(n=293)和 35 例健康志愿者(n=35)进行血浆 MIC-1、全身炎症(定义为血浆 C 反应蛋白(CRP)≥10mg/L 或改良格拉斯哥预后评分(mGPS)≥1)和营养状况评估。
与对照组相比(中位数=377pg/ml;范围 141-3786;P<0.001),患者的 MIC-1 水平升高(中位数=1371pg/ml;范围 141-39053)。胃肿瘤患者的 MIC-1 浓度高于交界处肿瘤患者(中位数=1592pg/ml;范围 141-12643)和食管肿瘤患者(中位数=1180pg/ml;范围 258-31184;P=0.015)。患者的体重平均减轻 6.4%(范围 0.0-33.4%),42%的患者 mGPS≥1 或血浆 CRP≥10mg/L(中位数=9mg/L;范围 1-200)。MIC-1 与疾病分期(r²=0.217;P<0.001)、年龄(r²=0.332;P<0.001)、CRP(r²=0.314;P<0.001)和 mGPS(r²=0.336;P<0.001)呈正相关,与卡氏功能状态评分(r²=-0.269;P<0.001)呈负相关。然而,尽管 MIC-1 与饮食摄入呈弱相关(r²=0.157;P=0.031),但与体重减轻、BMI 或人体测量学无关。MIC-1 水平处于上四分位的患者的生存率(中位数=204 天;95%CI 157-251)较 MIC-1 水平处于下三分位的患者(中位数=316 天;95%CI 259-373;P=0.036)降低,但 MIC-1 不是独立的预后指标。
在 OGC 中,血浆 MIC-1 水平与营养消耗状态或生存之间没有独立联系。