Department of Psychiatry, CES University, Medellín, Colombia.
Int J Neuropsychopharmacol. 2010 Jul;13(6):813-32. doi: 10.1017/S1461145709991246. Epub 2010 Feb 4.
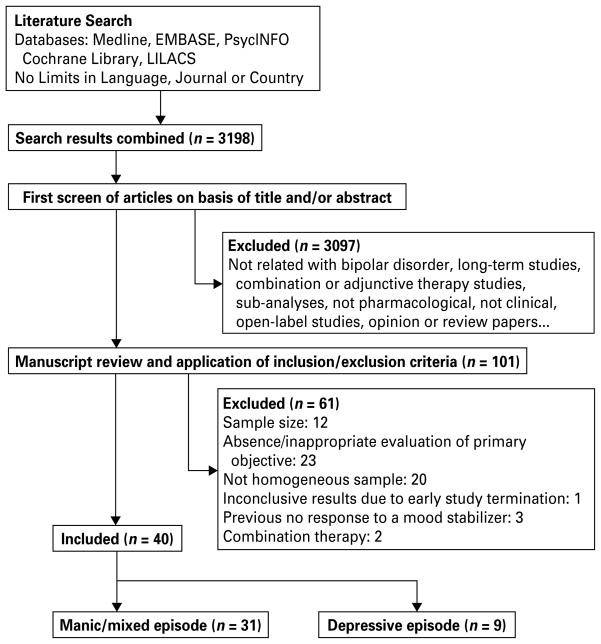
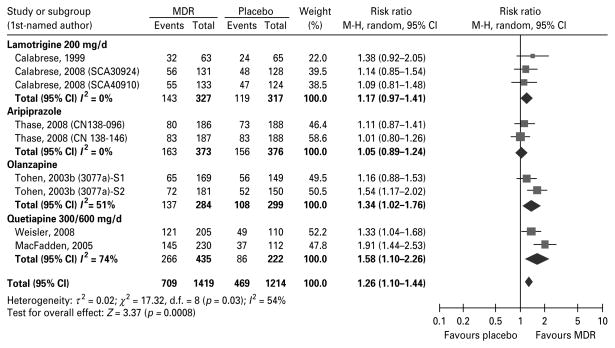
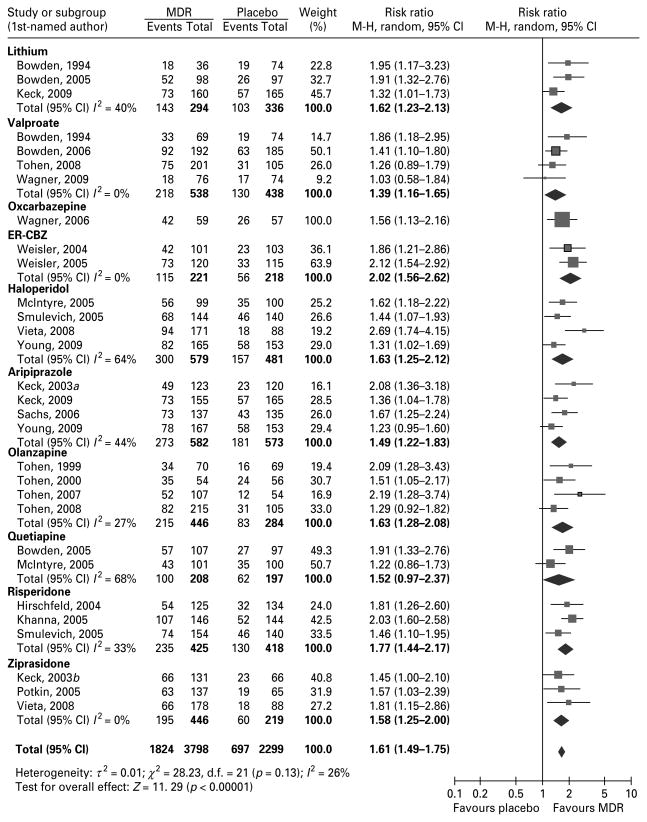
In recent years, combinations of pharmacological treatments have become common for the treatment of bipolar disorder type I (BP I); however, this practice is usually not evidence-based and rarely considers monotherapy drug regimen (MDR) as an option in the treatment of acute phases of BP I. Therefore, we evaluated comparative data of commonly prescribed MDRs for both manic and depressive phases of BP I. Medline, PsycINFO, EMBASE, the Cochrane Library, the ClinicalStudyResults.org and other data sources were searched from 1949 to March 2009 for placebo and active controlled randomized clinical trials (RCTs). Risk ratios (RRs) for response, remission, and discontinuation rates due to adverse events (AEs), lack of efficacy, or discontinuation due to any cause, and the number needed to treat or harm (NNT or NNH) were calculated for each medication individually and for all evaluable trials combined. The authors included 31 RCTs in the analyses comparing a MDR with placebo or with active treatment for acute mania, and 9 RCTs comparing a MDR with placebo or with active treatment for bipolar depression. According to the collected evidence, most of the MDRs when compared to placebo showed significant response and remission rates in acute mania. In the case of bipolar depression only quetiapine and, to a lesser extent, olanzapine showed efficacy as MDR. Overall, MDRs were well tolerated with low discontinuation rates due to any cause or AE, although AE profiles differed among treatments. We concluded that most MDRs were efficacious and safe in the treatment of manic episodes, but very few MDRs have demonstrated being efficacious for bipolar depressive episodes.
近年来,联合药物治疗已成为治疗 I 型双相情感障碍(BP I)的常用方法;然而,这种做法通常没有循证依据,很少将单药治疗方案(MDR)作为治疗 BP I 急性发作的选择。因此,我们评估了常用于治疗 BP I 躁狂和抑郁发作的常见 MDR 的对照数据。从 1949 年到 2009 年 3 月,我们在 Medline、PsycINFO、EMBASE、Cochrane 图书馆、ClinicalStudyResults.org 和其他数据源中搜索了安慰剂和活性对照随机临床试验(RCT)的对照数据。分别计算了每种药物和所有可评估试验联合治疗的反应、缓解和因不良反应(AE)、无效或因任何原因停药的停药率、治疗或危害所需的人数(NNT 或 NNH)的风险比(RR)。作者将 31 项 RCT 纳入了比较 MDR 与安慰剂或与活性治疗急性躁狂的分析,9 项 RCT 比较了 MDR 与安慰剂或与活性治疗双相抑郁的分析。根据收集到的证据,与安慰剂相比,大多数 MDR 在急性躁狂中显示出显著的反应和缓解率。在双相抑郁的情况下,只有喹硫平和在较小程度上奥氮平显示出作为 MDR 的疗效。总体而言,MDR 在治疗躁狂发作时耐受性良好,因任何原因或 AE 导致的停药率低,尽管治疗之间的 AE 谱不同。我们的结论是,大多数 MDR 在治疗躁狂发作时是有效和安全的,但很少有 MDR 被证明对双相抑郁发作有效。