Department of Internal Medicine, Pneumology and Allergology, Medical University of Warsaw, Warsaw, Poland.
Eur J Med Res. 2009 Dec 7;14 Suppl 4(Suppl 4):90-6. doi: 10.1186/2047-783x-14-s4-90.
Despite a number of important differences in the pathogenesis, course and prognosis of asthma and chronic obstructive pulmonary disease (COPD), these two entities also have common features with airway inflammation being one of them. Airway remodeling is a characteristic feature of asthma, but data on the bronchial wall thickening in COPD patients are still scarce.
To assess the relation between the inflammatory cell count in the bronchoalveolar lavage fluid (BALF) and thickness of bronchial walls assessed by high resolution computed tomography (HRCT) in asthma and COPD patients.
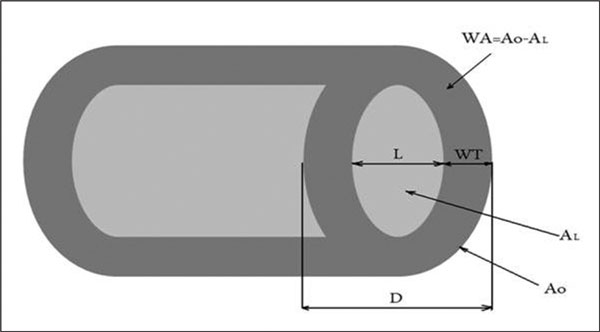
The study was conducted in 9 patients with mild-to-moderate asthma (M/F 4/5, mean age 35 +/- 10 years) and 11 patients with mild-to-moderate COPD (M/F 7/4, mean age 57 +/- 9 years). In all subjects lung function tests and HRCT scanning of the chest were performed. External (D) and internal (L) diameters of the airways were assessed at five selected lung levels. The lumen area (A(L)), wall area (WA), wall thickness (WT) and bronchial wall thickness (WT/D ratio) were calculated. Eight patients with asthma and 8 patients with COPD underwent fiberoptic bronchoscopy and bronchoalveolar lavage (BAL). Total and differential cell counts were assessed in the BAL fluid.
Mean FEV(1)% pred was 80 +/- 19%, and 73 +/- 20% in asthma and COPD patients, respectively (NS). No significant differences in the total and differential cell counts in BALF were found in patients with asthma and COPD. There were no significant differences in the airway diameter or airway wall thickness. The mean inner airway diameter was 1.4 +/- 0.3 and 1.2 +/- 0.3 mm and the mean lumen area was 1.8 +/- 0.7 and 1.6 +/- 0.7 mm(2) in asthma and COPD, respectively (NS). Negative correlations between the eosinophil count in BALF and inner airway diameter (r=-0.7, P<0.05) and lumen area (r=-0.7, P<0.05) were found in asthmatics. There was no significant relationship between the BALF cell count and airway wall thickness in COPD patients. -
In mild-to-moderate asthma and COPD the airway diameter and thickness are similar. In asthmatics, the airway diameter might be associated with eosinophil count in BAL fluid.
评估支气管肺泡灌洗液(BALF)中炎症细胞计数与哮喘和 COPD 患者高分辨率 CT(HRCT)评估的支气管壁厚度之间的关系。
本研究纳入 9 名轻中度哮喘患者(男女比例 4/5,平均年龄 35 ± 10 岁)和 11 名轻中度 COPD 患者(男女比例 7/4,平均年龄 57 ± 9 岁)。所有患者均进行了肺功能检查和胸部 HRCT 扫描。在五个选定的肺水平评估气道的外部(D)和内部(L)直径。计算管腔面积(A(L))、壁面积(WA)、壁厚度(WT)和支气管壁厚度(WT/D 比)。8 例哮喘患者和 8 例 COPD 患者接受纤维支气管镜检查和支气管肺泡灌洗(BAL)。评估 BAL 液中的总细胞计数和分类细胞计数。
FEV(1)%预计值平均为 80 ± 19%,哮喘和 COPD 患者分别为 73 ± 20%(无统计学差异)。哮喘和 COPD 患者 BALF 中的总细胞计数和分类细胞计数无显著差异。气道直径或气道壁厚度无显著差异。平均内气道直径分别为 1.4 ± 0.3 和 1.2 ± 0.3mm,平均管腔面积分别为 1.8 ± 0.7 和 1.6 ± 0.7mm(2)在哮喘和 COPD 中,差异无统计学意义(NS)。哮喘患者 BAL 中嗜酸性粒细胞计数与内气道直径(r=-0.7,P<0.05)和管腔面积(r=-0.7,P<0.05)呈负相关。COPD 患者 BALF 细胞计数与气道壁厚度无显著相关性。
在轻中度哮喘和 COPD 中,气道直径和厚度相似。在哮喘患者中,气道直径可能与 BAL 液中的嗜酸性粒细胞计数相关。