Department of Neurology and Clinical Neurophysiology, Academic Medical Centre, Amsterdam, The Netherlands.
Exp Brain Res. 2010 May;202(3):681-91. doi: 10.1007/s00221-010-2174-x. Epub 2010 Feb 16.
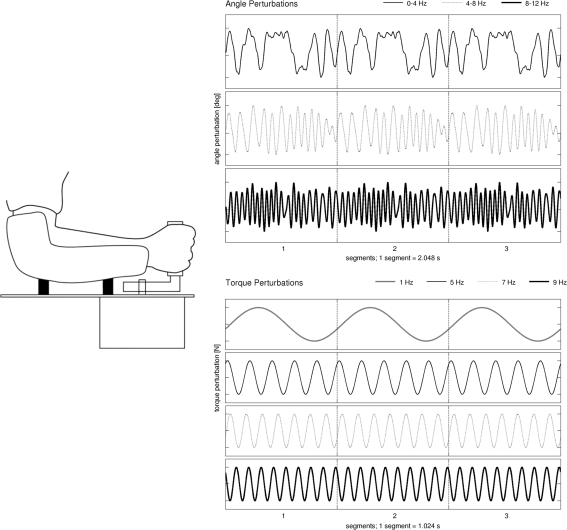
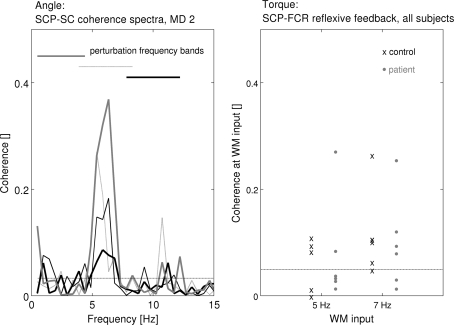
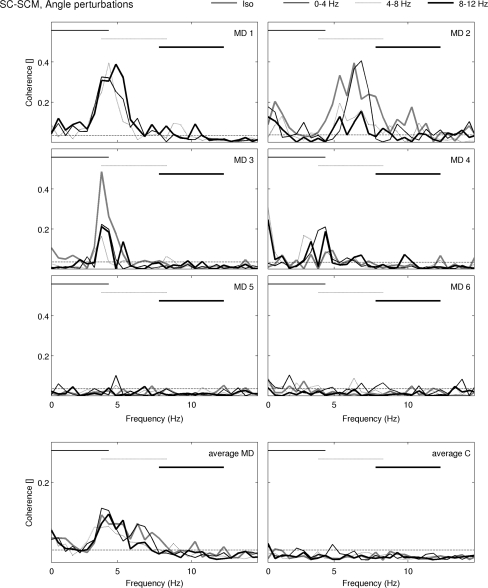
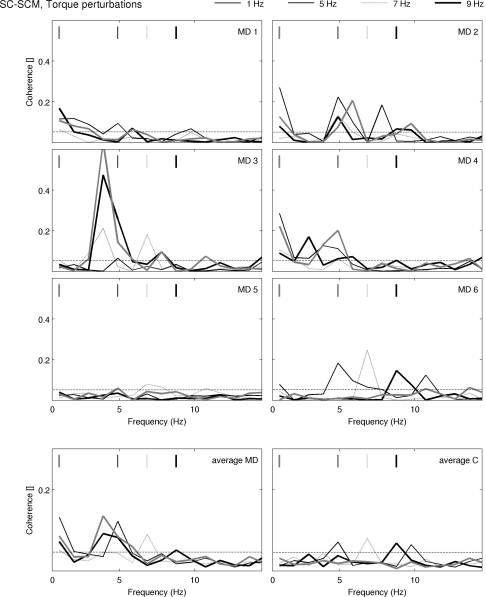
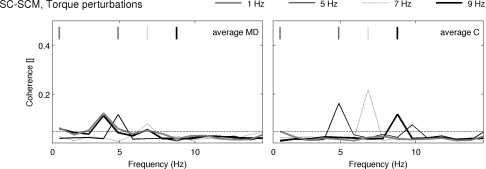
In dystonia, both sensory malfunctioning and an abnormal intermuscular low-frequency drive of 3-7 Hz have been found, although cause and effect are unknown. It is hypothesized that sensory processing is primarily disturbed and induces this drive. Accordingly, experimenter-controlled sensory input should be able to influence the frequency of the drive. In six genetically confirmed myoclonus-dystonia (MD) patients and six matched controls, the low-frequency drive was studied with intermuscular coherence analysis. External perturbations were applied mechanically to the wrist joint in small frequency bands (0-4, 4-8 and 8-12 Hz; 'angle' protocol) and at single frequencies (1, 5, 7 and 9 Hz; 'torque' protocol). The low-frequency drive was found in the neck muscles of 4 MD patients. In these patients, its frequency did not shift due to the perturbation. In the torque protocol, the externally applied frequencies could be detected in all controls and in the two patients without the common drive. The common low-frequency drive was not be affected by external perturbations in MD patients. Furthermore, the torque protocol did not induce intermuscular coherences at the applied frequencies in these patients, as was the case in healthy controls and in patients without the drive. This suggests that the dystonic 3-7 Hz drive is caused by a sensory-independent motor drive and sensory malfunctioning in MD might rather be a consequence than a cause of dystonia.
在肌张力障碍中,已经发现了感觉功能障碍和 3-7 Hz 的异常肌肉间低频驱动,尽管原因和结果尚不清楚。据推测,感觉处理主要受到干扰,并引起这种驱动。因此,实验者控制的感觉输入应该能够影响驱动的频率。在 6 名经基因证实的肌阵挛-肌张力障碍 (MD) 患者和 6 名匹配的对照者中,使用肌肉间相干性分析研究了低频驱动。外部扰动以小频带(0-4、4-8 和 8-12 Hz;“角度”协议)和单频(1、5、7 和 9 Hz;“扭矩”协议)机械施加到手关节。低频驱动在 4 名 MD 患者的颈部肌肉中被发现。在这些患者中,由于扰动,其频率没有改变。在扭矩协议中,所有对照者和没有共同驱动的两名患者都可以检测到外部施加的频率。共同的低频驱动不会被 MD 患者的外部扰动所影响。此外,在这些患者中,扭矩协议没有在应用频率下引起肌肉间相干性,而健康对照者和没有驱动的患者则存在这种情况。这表明,肌张力障碍的 3-7 Hz 驱动是由一种感觉独立的运动驱动引起的,而 MD 中的感觉功能障碍更可能是肌张力障碍的结果而不是原因。