Sexual Health Unit, Melbourne School of Population Health, The University of Melbourne, Carlton, Victoria 3053, Australia.
BMC Public Health. 2010 Feb 17;10:70. doi: 10.1186/1471-2458-10-70.
Financial incentives have been used for many years internationally to improve quality of care in general practice. The aim of this pilot study was to determine if offering general practitioners (GP) a small incentive payment per test would increase chlamydia testing in women aged 16 to 24 years, attending general practice.
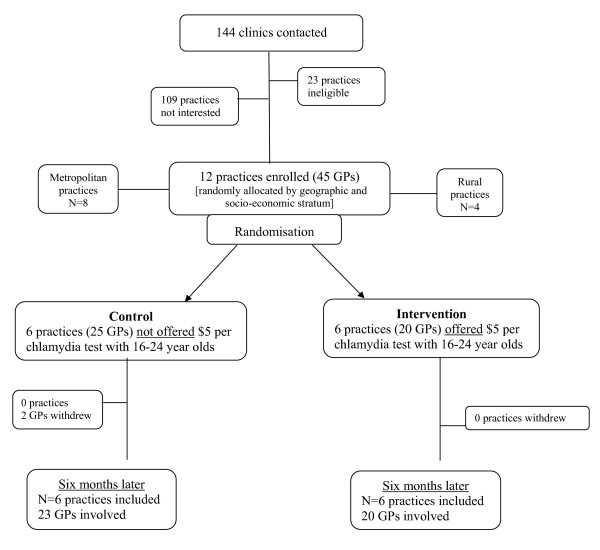
General practice clinics (n = 12) across Victoria, Australia, were cluster randomized to receive either a $AUD5 payment per chlamydia test or no payment for testing 16 to 24 year old women for chlamydia. Data were collected on the number of chlamydia tests and patient consultations undertaken by each GP over two time periods: 12 month pre-trial and 6 month trial period. The impact of the intervention was assessed using a mixed effects logistic regression model, accommodating for clustering at GP level.
Testing increased from 6.2% (95% CI: 4.2, 8.4) to 8.8% (95% CI: 4.8, 13.0) (p = 0.1) in the control group and from 11.5% (95% CI: 4.6, 18.5) to 13.4% (95% CI: 9.5, 17.5) (p = 0.4) in the intervention group. Overall, the intervention did not result in a significant increase in chlamydia testing in general practice. The odds ratio for an increase in testing in the intervention group compared to the control group was 0.9 (95% CI: 0.6, 1.2). Major barriers to increased chlamydia testing reported by GPs included a lack of time, difficulty in remembering to offer testing and a lack of patient awareness around testing.
A small financial incentive alone did not increase chlamydia testing among young women attending general practice. It is possible small incentive payments in conjunction with reminder and feedback systems may be effective, as may higher financial incentive payments. Further research is required to determine if financial incentives can increase testing in Australian general practice, the type and level of financial scheme required and whether incentives needs to be part of a multi-faceted package.
Australian New Zealand Clinical Trial Registry ACTRN12608000499381.
国际上多年来一直使用经济激励措施来提高一般实践中的医疗质量。本试点研究的目的是确定向全科医生(GP)提供每次检测的少量激励性报酬是否会增加对 16 至 24 岁女性进行衣原体检测的数量,这些女性在一般实践中就诊。
澳大利亚维多利亚州的全科诊所(n=12)采用整群随机分组,分别接受每次衣原体检测 5 澳元的报酬或不支付报酬,以检测 16 至 24 岁的女性是否患有衣原体。在两个时间段内收集每位 GP 进行的衣原体检测和患者就诊的数量:试验前 12 个月和 6 个月的试验期。使用混合效应逻辑回归模型评估干预的影响,同时考虑 GP 层面的聚类。
对照组的检测率从 6.2%(95%CI:4.2,8.4)增加到 8.8%(95%CI:4.8,13.0)(p=0.1),干预组从 11.5%(95%CI:4.6,18.5)增加到 13.4%(95%CI:9.5,17.5)(p=0.4)。总体而言,该干预措施并未导致一般实践中衣原体检测的显著增加。与对照组相比,干预组检测增加的优势比为 0.9(95%CI:0.6,1.2)。GP 报告的增加衣原体检测的主要障碍包括时间不足、难以记住提供检测以及患者对检测的认识不足。
仅提供少量经济激励措施并不能增加年轻女性在一般实践中进行衣原体检测的数量。可能需要结合提醒和反馈系统的小额激励支付,或者更高的经济激励支付,才可能有效。需要进一步研究以确定经济激励措施是否可以增加澳大利亚一般实践中的检测数量,需要哪种类型和水平的财务计划,以及激励措施是否需要成为多方面方案的一部分。
澳大利亚新西兰临床试验注册中心 ACTRN12608000499381。