Department Medical Oncology, Charing Cross Hospital Trophoblastic Disease Screening and Treatment Centre, Imperial College NHS Healthcare Trust, Fulham Palace Road, London, UK.
Br J Cancer. 2010 Mar 2;102(5):810-4. doi: 10.1038/sj.bjc.6605529. Epub 2010 Feb 16.
Gestational trophoblastic neoplasia (GTN) after a hydatidiform mole is either treated with single- or multi-agent chemotherapy determined by a multifactorial scoring system. Women with human chorionic gonadotrophin (hCG) levels >100 000 IU l(-1) can remain within the low-risk/single-agent category and usually choose one drug therapy. Here we compare the success and duration of single- vs multi-agent chemotherapy in this patient group.
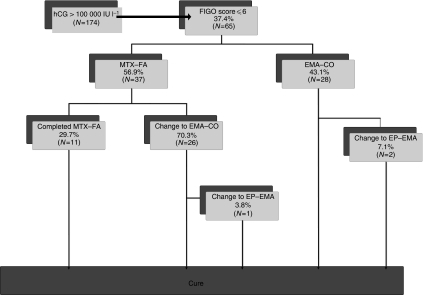
Between 1980 and 2008, 65 women had a pre-treatment hCG >100 000 IU l(-1) and were low risk. The initial hCG level, treatment regimens, changes and duration and overall survival were recorded.
Of 37 patients starting low-risk/single-agent treatment, 11 (29.7%) were treated successfully, whereas 26 (70.3%) required additional multi-agent chemotherapy to achieve complete remission (CR). Combination chemotherapy was initially commenced in 28 women, and 2 (7%) required additional drugs for CR. The overall duration of therapy for those commencing and completing single- or multi-agent chemotherapy was 130 and 123 days (P=0.78), respectively. The median-treatment duration for patients commencing single-agent but changing to multi-agent chemotherapy was 13 days more than those receiving high-risk treatment alone (136 vs 123 days; P=0.07). All 3 patients with an initial hCG >400 000 IU l(-1) and treated with single-agent therapy developed drug resistance. Overall survival for all patients was 100%.
Low-risk post-molar GTN patients with a pre-treatment hCG >100 000 and <400 000 IU l(-1) can be offered low-risk single-agent therapy, as this will cure 30%, is relatively non-toxic and only prolongs treatment by 2 weeks if a change to combination agents is required. Patients whose hCG is >400 000 IU l(-1) should receive multi-agent chemotherapy from the outset.
葡萄胎后发生的妊娠滋养细胞肿瘤(GTN)根据多因素评分系统采用单一或多种药物化疗进行治疗。hCG 水平>100000IU/L 的女性可归入低危/单一药物治疗类别,通常选择一种药物治疗。在此,我们比较该患者人群中单一药物与多种药物化疗的成功率和持续时间。
1980 年至 2008 年间,有 65 名患者治疗前 hCG>100000IU/L 且为低危。记录初始 hCG 水平、治疗方案、变化和持续时间以及总生存情况。
37 名开始低危/单一药物治疗的患者中,11 名(29.7%)治疗成功,而 26 名(70.3%)需要额外的多种药物化疗才能达到完全缓解(CR)。28 名女性最初开始联合化疗,2 名(7%)需要额外药物才能达到 CR。开始单一或多种药物化疗并完成治疗的患者的总治疗时间分别为 130 天和 123 天(P=0.78)。开始单一药物治疗但转为联合药物治疗的患者的中位治疗时间比单独接受高危治疗的患者多 13 天(136 天 vs 123 天;P=0.07)。所有 3 名初始 hCG>400000IU/L 且接受单一药物治疗的患者均出现耐药。所有患者的总生存率为 100%。
对于初始 hCG>100000 且<400000IU/L 的低危葡萄胎后 GTN 患者,可以提供低危的单一药物治疗,因为这将治愈 30%的患者,且相对无毒,只有在需要转为联合药物治疗时才会延长治疗时间 2 周。hCG>400000IU/L 的患者应从一开始就接受多种药物化疗。