Department of Obstetrics and Gynecology, Gestational Trophoblastic Disease Unit, Hospital Universitario de Caracas, Universidad Central de Venezuela, Caracas, Venezuela.
Department of Medical Oncology, Gestational Trophoblastic Disease Centre, Imperial College Healthcare NHS Trust, Charing Cross Hospital, London, UK.
ESMO Open. 2021 Jun;6(3):100110. doi: 10.1016/j.esmoop.2021.100110. Epub 2021 Apr 10.
A human chorionic gonadotropin (hCG) cut-off of ≤300 IU/l for starting actinomycin D (ActD) in post-molar gestational trophoblastic neoplasia (GTN) patients developing methotrexate resistance (MTX-R) reduced the number of women needing toxic multi-agent chemotherapy (etoposide, MTX and ActD alternating weekly with cyclophosphamide and vincristine; EMA/CO) without affecting survival. Here we assess whether an increased hCG cut-off of ≤1000 IU/l spares more women EMA/CO.
All post-molar GTN patients treated with first-line methotrexate and folinic acid (MTX/FA) were identified in a national cohort between 2009 and 2016. Data collected included age, FIGO score, the hCG levels at MTX-R, and treatment outcomes.
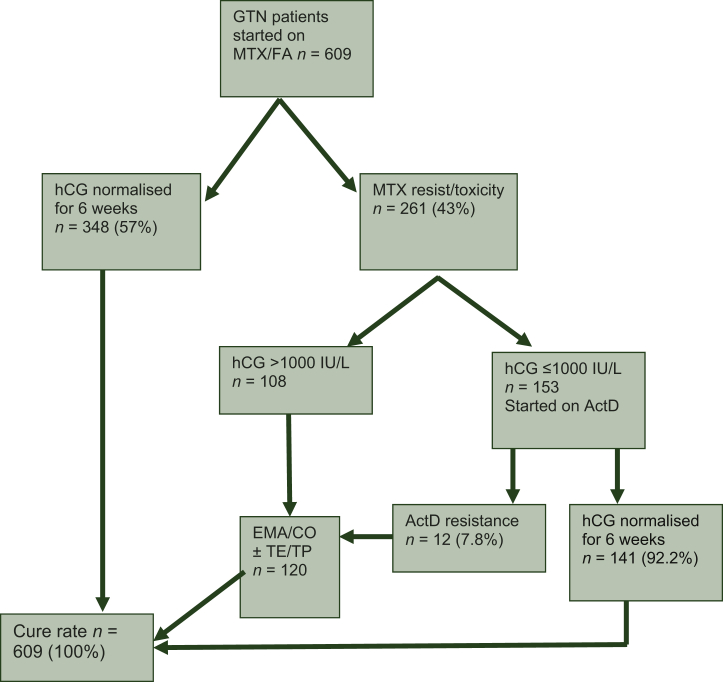
In total, 609 GTN patients commenced treatment with MTX/FA achieving a complete response in 57% (348/609). Resistance developed in 25.1% (153/609) at an hCG ≤ 1000 IU/l and switching to ActD achieved remission in 92.8% without any major toxicity with the remaining 7.2% remitting on EMA/CO. Comparative analysis of patients switching at an hCG <100 versus 100-300 versus 300-1000 IU/l revealed a significant fall in the cure rate with second-line ActD from 97% (93/96) to 87% (34/39) to 78% (14/18), respectively, P = 0.009. However, by increasing the hCG cut-off from ≤300 to ≤1000 IU/l, 14 patients were spared EMA/CO chemotherapy. Moreover, in the present series, all post-molar GTN remain in remission.
This study demonstrates that increasing the hCG cut-off from ≤300 to ≤1000 IU/l for choosing patients for ActD following MTX-R spares more women with GTN from the greater toxicity of EMA/CO without compromising 100% survival outcomes.
在人绒毛膜促性腺激素(hCG) cutoff 值≤300IU/l 时开始使用放线菌素 D(ActD)治疗发生甲氨蝶呤耐药(MTX-R)的绒毛膜癌(GTN)患者,可减少需要接受毒性更大的多药物化疗(依托泊苷、甲氨蝶呤和 ActD 每周交替与环磷酰胺和长春新碱;EMA/CO)的女性数量,而不影响生存率。在此,我们评估 hCG cutoff 值增加至≤1000IU/l 是否可以使更多的患者免于接受 EMA/CO 治疗。
在 2009 年至 2016 年间,我们在一个全国性队列中确定了所有接受一线甲氨蝶呤和叶酸(MTX/FA)治疗的绒毛膜癌患者。收集的数据包括年龄、FIGO 评分、MTX-R 时的 hCG 水平以及治疗结局。
共有 609 例 GTN 患者开始接受 MTX/FA 治疗,其中 57%(348/609)患者完全缓解。在 hCG≤1000IU/l 时,25.1%(153/609)患者发生耐药,改用 ActD 后,92.8%的患者缓解,没有发生严重毒性反应,其余 7.2%的患者在接受 EMA/CO 治疗后缓解。对 hCG<100IU/l、100-300IU/l 和 300-1000IU/l 时切换至 ActD 的患者进行比较分析显示,二线 ActD 的治愈率显著下降,分别为 97%(93/96)、87%(34/39)和 78%(14/18),P=0.009。然而,通过将 hCG cutoff 值从≤300IU/l 增加到≤1000IU/l,14 例患者免于接受 EMA/CO 化疗。此外,在本系列中,所有绒毛膜癌患者仍处于缓解状态。
本研究表明,在 MTX-R 后选择 ActD 治疗时,将 hCG cutoff 值从≤300IU/l 增加到≤1000IU/l,可以使更多的 GTN 患者避免接受 EMA/CO 化疗的更大毒性,而不影响 100%的生存结局。