Department of Public Health and Policy, London School of Hygiene and Tropical Medicine, London, UK.
Sex Transm Infect. 2010 Feb;86 Suppl 1(Suppl_1):i89-94. doi: 10.1136/sti.2009.038547.
The India AIDS Initiative (Avahan) project is involved in rapid scale-up of HIV-prevention interventions in high-risk populations. This study examines the cost variation of 107 non-governmental organisations (NGOs) implementing targeted interventions, over the start up (defined as period from project inception until services to the key population commenced) and first 2 years of intervention.
The Avahan interventions for female and male sex workers and their clients, in 62 districts of four southern states were costed for the financial years 2004/2005 and 2005/2006 using standard costing techniques. Data sources include financial and economic costs from the lead implementing partners (LPs) and subcontracted local implementing NGOs retrospectively and prospectively collected from a provider perspective. Ingredients and step-down allocation processes were used. Outcomes were measured using routinely collected project data. The average costs were estimated and a regression analysis carried out to explore causes of cost variation. Costs were calculated in US$ 2006.
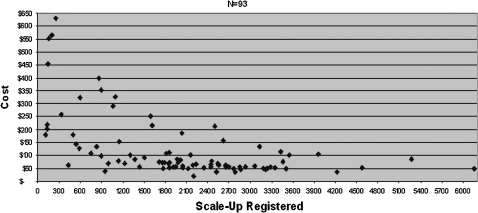
The total number of registered people was 134,391 at the end of 2 years, and 124,669 had used STI services during that period. The median average cost of Avahan programme for this period was $76 per person registered with the project. Sixty-one per cent of the cost variation could be explained by scale (positive association), number of NGOs per district (negative), number of LPs in the state (negative) and project maturity (positive) (p<0.0001).
During rapid scale-up in the initial phase of the Avahan programme, a significant reduction in average costs was observed. As full scale-up had not yet been achieved, the average cost at scale is yet to be realised and the extent of the impact of scale on costs yet to be captured. Scale effects are important to quantify for planning resource requirements of large-scale interventions. The average cost after 2 years is within the range of global scale-up costs estimates and other studies in India.
印度艾滋病倡议(Avahan)项目参与了高危人群中艾滋病毒预防干预措施的快速推广。本研究考察了在启动阶段(定义为项目启动至向重点人群提供服务开始)和干预的头两年,107 个实施针对性干预措施的非政府组织(NGO)的成本差异。
使用标准成本核算技术,对来自四个南部邦的 62 个地区的男、女性工作者及其客户的 Avahan 干预措施进行了核算,核算所依据的是 2004/2005 年和 2005/2006 年的财政年度数据。数据来源包括从主要实施伙伴(LP)和分包的当地实施 NGO 收集的财务和经济成本,从提供者的角度进行回顾性和前瞻性收集。使用配料和逐步分配过程。使用常规收集的项目数据来衡量结果。对平均成本进行了估计,并进行了回归分析以探讨成本差异的原因。成本按 2006 年美元计算。
在两年结束时,注册人数达到 134391 人,在此期间有 124669 人使用了性传播感染服务。在此期间,该项目的艾滋病倡议方案的平均成本中位数为每人 76 美元。61%的成本差异可以用规模(正相关)、每个区的 NGO 数量(负相关)、邦内的 LP 数量(负相关)和项目成熟度(正相关)来解释(p<0.0001)。
在艾滋病倡议项目初始阶段的快速推广阶段,观察到平均成本显著降低。由于尚未实现全面推广,因此尚未实现全面推广的平均成本,尚未捕捉到规模对成本的影响程度。规模效应对于量化大规模干预措施的资源需求非常重要。两年后的平均成本在全球推广成本估计和印度其他研究的范围内。