Anderson Sarah-Jane, Ghys Peter D, Ombam Regina, Hallett Timothy B
Department of Infectious Disease Epidemiology, Imperial College London, London, UK.
UNAIDS, Geneva, Switzerland.
J Int AIDS Soc. 2017 Dec;20(4). doi: 10.1002/jia2.25020.
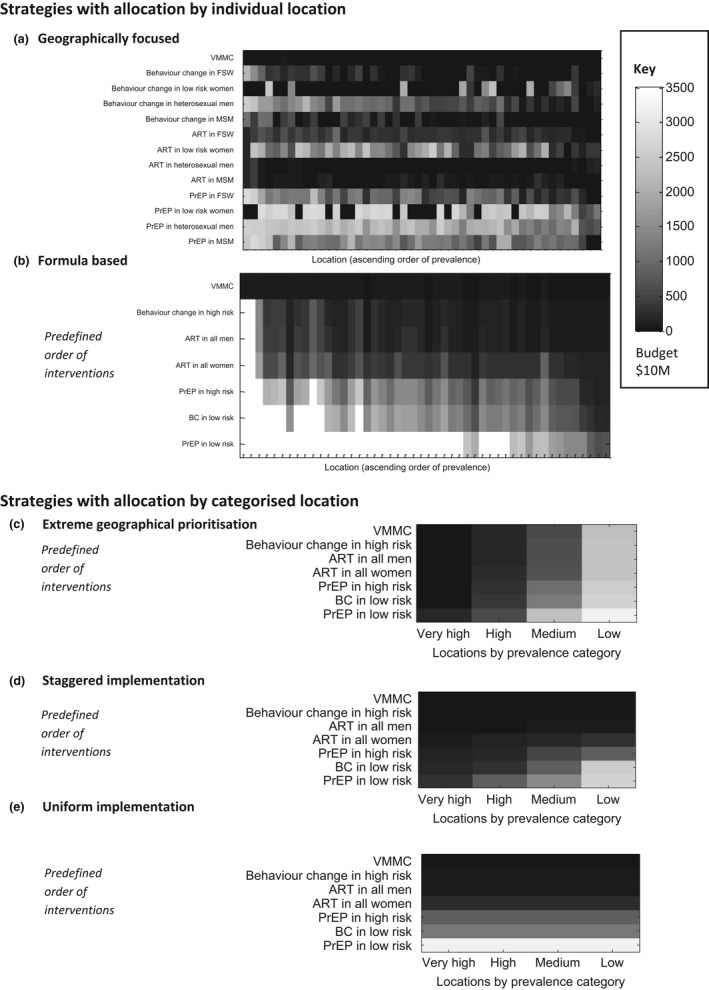
A strategic approach to the application of HIV prevention interventions is a core component of the UNAIDS Fast Track strategy to end the HIV epidemic by 2030. Central to these plans is a focus on high-prevalence geographies, in a bid to target resources to those in greatest need and maximize the reduction in new infections. Whilst this idea of geographical prioritization has the potential to improve efficiency, it is unclear how it should be implemented in practice. There are a range of prevention interventions which can be applied differentially across risk groups and locations, making allocation decisions complex. Here, we use mathematical modelling to compare the impact (infections averted) of a number of different approaches to the implementation of geographical prioritization of prevention interventions, similar to those emerging in policy and practice, across a range of prevention budgets.
We use geographically specific mathematical models of the epidemic and response in 48 counties and major cities of Kenya to project the impact of the different geographical prioritization approaches. We compare the geographical allocation strategies with a nationally uniform approach under which the same interventions must be applied across all modelled locations.
We find that the most extreme geographical prioritization strategy, which focuses resources exclusively to high-prevalence locations, may substantially restrict impact (41% fewer infections averted) compared to a nationally uniform approach, as opportunities for highly effective interventions for high-risk populations in lower-prevalence areas are missed. Other geographical allocation approaches, which intensify efforts in higher-prevalence areas whilst maintaining a minimum package of cost-effective interventions everywhere, consistently improve impact at all budget levels. Such strategies balance the need for greater investment in locations with the largest epidemics whilst ensuring higher-risk groups in lower-priority locations are provided with cost-effective interventions.
Our findings serve as a warning to not be too selective in the application of prevention strategies. Further research is needed to understand how decision-makers can find the right balance between the choice of interventions, focus on high-risk populations, and geographical targeting to ensure the greatest impact of HIV prevention.
采用战略方法应用艾滋病预防干预措施是联合国艾滋病规划署到2030年终结艾滋病流行的快速通道战略的核心组成部分。这些计划的核心是关注高流行地区,以便将资源投向最需要的人群,并最大限度地减少新感染病例。虽然这种地理优先排序的理念有可能提高效率,但在实践中应如何实施尚不清楚。有一系列预防干预措施可根据风险群体和地点的不同而有所差异地应用,这使得分配决策变得复杂。在此,我们使用数学模型来比较多种不同的预防干预措施地理优先排序实施方法(类似于政策和实践中出现的方法)在一系列预防预算下的影响(避免的感染病例数)。
我们使用肯尼亚48个县和主要城市的疫情及应对措施的地理特定数学模型,来预测不同地理优先排序方法的影响。我们将地理分配策略与全国统一方法进行比较,在全国统一方法下,必须在所有建模地点应用相同的干预措施。
我们发现,与全国统一方法相比,最极端的地理优先排序策略(即将资源仅集中于高流行地区)可能会大幅限制影响(避免的感染病例数减少41%),因为会错过在低流行地区对高风险人群进行高效干预的机会。其他地理分配方法,即在高流行地区加大力度,同时在各地维持一套最低限度的具有成本效益的干预措施,在所有预算水平上都能持续提高影响。这些策略在对疫情最严重地区加大投资的需求与确保为低优先级地区的高风险群体提供具有成本效益的干预措施之间取得了平衡。
我们的研究结果警示人们,在应用预防策略时不要过于有选择性。需要进一步开展研究,以了解决策者如何在干预措施的选择、对高风险人群的关注以及地理定位之间找到正确的平衡,以确保艾滋病预防产生最大影响。