Department of Gastroenterology and Hepatology, University Medical Center Utrecht, Heidelberglaan 100, 3584 CX, Utrecht, The Netherlands.
Surg Endosc. 2010 Sep;24(9):2260-7. doi: 10.1007/s00464-010-0946-9. Epub 2010 Feb 23.
Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) of mediastinal lymphadenopathy has been shown to be a valuable diagnostic tool in high-volume EUS centers (≥ 50 mediastinal EUS-FNA/endoscopist/year). Our goal was to assess the diagnostic accuracy of EUS-FNA and its impact on clinical management and costs in low-volume EUS centers (<50 mediastinal EUS-FNA/endoscopist/year).
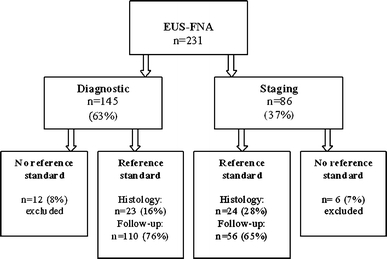
Consecutive patients referred to two Dutch endoscopy centers in the period 2002-2008 for EUS-FNA of mediastinal lymphadenopathy were reviewed. The gold standard for a cytological diagnosis was histological confirmation or clinical follow-up of more than 6 months with repeat imaging. The impact of EUS-FNA on clinical management was subdivided into a positive impact by providing (1) adequate cytology that influenced the decision to perform surgery or (2) a diagnosis of a benign inflammatory disorder, and a negative impact which was subdivided into (1) false-negative or inconclusive cytology or (2) an adequate cytological diagnosis that did not influence patient management. Costs of an alternative diagnostic work-up without EUS-FNA, as established by an expert panel, were compared to costs of the actual work-up.
In total, 213 patients (71% male, median age= 61 years, range = 23-88 years) underwent EUS-FNA. Sensitivity, specificity, and negative and positive predictive values were 89%, 100%, 80%, and 100%, respectively. EUS-FNA had a positive impact on clinical management in 84% of cases by either influencing the decision to perform surgery (49%) or excluding malignant lymphadenopathy (35%), and a negative impact in 7% of cases because of inadequate (3%) or false-negative (4%) cytology. In 9% of cases, EUS-FNA was performed without an established indication. Two nonfatal perforations occurred (0.9%). Total cost reduction was €100,593, with a mean cost reduction of €472 (SD = €607) per patient.
Mediastinal EUS-FNA can be performed in low-volume EUS centers without compromising diagnostic accuracy. Moreover, EUS-FNA plays an important role in the management of patients with mediastinal lymphadenopathy and reduces total diagnostic costs.
在大容量内镜超声中心(≥50 例纵隔内镜超声引导细针抽吸术/内镜医师/年)中,内镜超声引导下细针抽吸术(EUS-FNA)对纵隔淋巴结病的诊断已被证明是一种有价值的诊断工具。我们的目标是评估低容量内镜超声中心(<50 例纵隔内镜超声引导细针抽吸术/内镜医师/年)中 EUS-FNA 的诊断准确性及其对临床管理和成本的影响。
回顾了 2002 年至 2008 年间荷兰两家内镜中心连续就诊的 213 例纵隔淋巴结病行 EUS-FNA 的患者。细胞学诊断的金标准为组织学证实或临床随访超过 6 个月并重复影像学检查。EUS-FNA 对临床管理的影响分为通过提供(1)足够的细胞学结果来影响手术决策或(2)诊断为良性炎症性疾病的积极影响,以及分为(1)假阴性或不确定的细胞学结果或(2)不影响患者管理的足够细胞学诊断的消极影响。与没有 EUS-FNA 的替代诊断方案相比,专家小组确定了该方案的成本,并将其与实际诊断方案的成本进行了比较。
总共 213 例患者(71%为男性,中位年龄为 61 岁,范围为 23-88 岁)接受了 EUS-FNA。敏感性、特异性、阴性预测值和阳性预测值分别为 89%、100%、80%和 100%。EUS-FNA 在 84%的病例中对临床管理有积极影响,要么通过影响手术决策(49%),要么排除恶性淋巴结病(35%),在 7%的病例中有负面影响,因为细胞学结果不足(3%)或假阴性(4%)。在 9%的病例中,EUS-FNA 是在没有明确适应证的情况下进行的。发生了 2 例非致命性穿孔(0.9%)。总费用降低了 100,593 欧元,平均每位患者降低了 472 欧元(标准差=607 欧元)。
在不影响诊断准确性的情况下,低容量内镜超声中心也可以进行纵隔 EUS-FNA。此外,EUS-FNA 在纵隔淋巴结病患者的管理中发挥了重要作用,并降低了总诊断成本。