Barr H, Chatlani P, Tralau C J, MacRobert A J, Boulos P B, Bown S G
National Medical Laser Centre, Department of Surgery, Rayne Institute, London.
Gut. 1991 May;32(5):517-23. doi: 10.1136/gut.32.5.517.
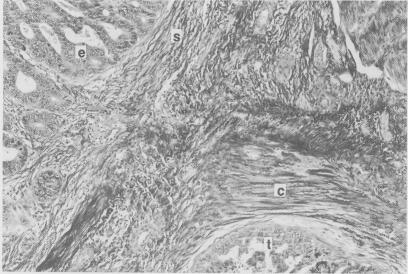
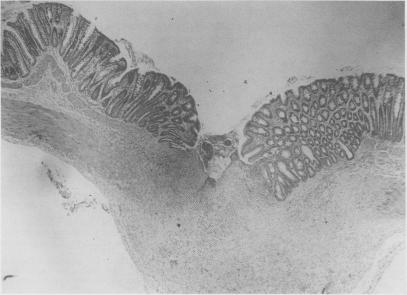
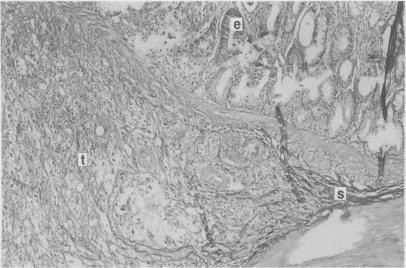
Photodynamic therapy is a photochemical technique for the local destruction of tumours, entailing the interaction of light with an administered photosensitiser to produce a cytotoxic effect. We investigated the tissue distribution of the photosensitiser aluminium sulphonated phthalocyanine (AlSPc) in dimethylhydrazine induced colonic tumours and adjacent normal colon in rats. Forty eight hours after intravenous injection, most tumours contained twice as much AlSPc as normal colon. Tumour size and position in the colon did not affect AlSPc concentration. Microscopic fluorescence localisation of AlSPc showed significant photosensitiser accumulation in tumour stroma, whereas tumour and normal mucosa contained similar amounts. Thus, some normal tissue damage, where malignant cells invade normal areas, would inevitably accompany eradication of tumours. Tumour destruction and healing of colon after tumour eradication were examined histologically. There was sharp demarcation between necrotic areas (tumour or normal) and adjacent tissue and, whether the treated area was tumour or normal, healing occurred by regeneration of normal tissue. Some incompletely eradicated large tumours showed evidence of delayed bleeding. The possibility of selective uptake or preferential retention of the photosensitiser in tumours formed the initial basis for investigation of photodynamic therapy, but it is now clear that this is seldom the most important factor for tumour eradication. Of far greater importance is the nature of the biological effect of photodynamic therapy as necrosis of small tumours involving the full thickness of the bowel wall can be achieved with safe healing by regeneration of normal colon. The maximum depth of necrosis produced was only a few millimetres, so this technique is unlikely to be of value as the primary treatment for large colonic tumours but may prove of value for eradicating small lesions or as adjunctive therapy for eradication of small nests of tumour remaining or recurring in the tumour bed after conventional surgery.
光动力疗法是一种用于局部破坏肿瘤的光化学技术,它需要光与所给予的光敏剂相互作用以产生细胞毒性作用。我们研究了磺化铝酞菁(AlSPc)这种光敏剂在二甲基肼诱导的大鼠结肠肿瘤及相邻正常结肠组织中的分布情况。静脉注射48小时后,大多数肿瘤中的AlSPc含量是正常结肠的两倍。肿瘤大小和在结肠中的位置并不影响AlSPc浓度。AlSPc的显微荧光定位显示,光敏剂在肿瘤基质中有显著积聚,而肿瘤和正常黏膜中的含量相似。因此,在根除肿瘤时,当恶性细胞侵入正常区域时,不可避免地会伴随一些正常组织的损伤。通过组织学检查了肿瘤破坏情况以及肿瘤根除后结肠的愈合情况。坏死区域(肿瘤或正常组织)与相邻组织之间有明显界限,且无论治疗区域是肿瘤还是正常组织,愈合都是通过正常组织的再生实现的。一些未完全根除的大肿瘤有延迟出血的迹象。光敏剂在肿瘤中选择性摄取或优先保留的可能性构成了光动力疗法研究的最初基础,但现在很清楚,这很少是根除肿瘤的最重要因素。更为重要的是光动力疗法的生物学效应的性质,因为通过正常结肠的再生实现安全愈合,可以使累及肠壁全层的小肿瘤发生坏死。产生的坏死最大深度仅为几毫米,所以这项技术作为大的结肠肿瘤的主要治疗方法可能没有价值,但对于根除小病变或作为传统手术后肿瘤床中残留或复发的小肿瘤巢的辅助治疗可能证明是有价值的。