Service d'épidémiologie et santé publique, Centre Hospitalier Universitaire, Rennes, France.
Brain. 2010 Jul;133(Pt 7):1900-13. doi: 10.1093/brain/awq076. Epub 2010 Apr 27.
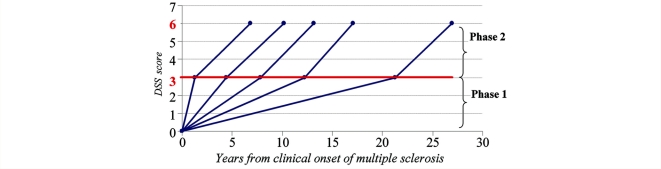
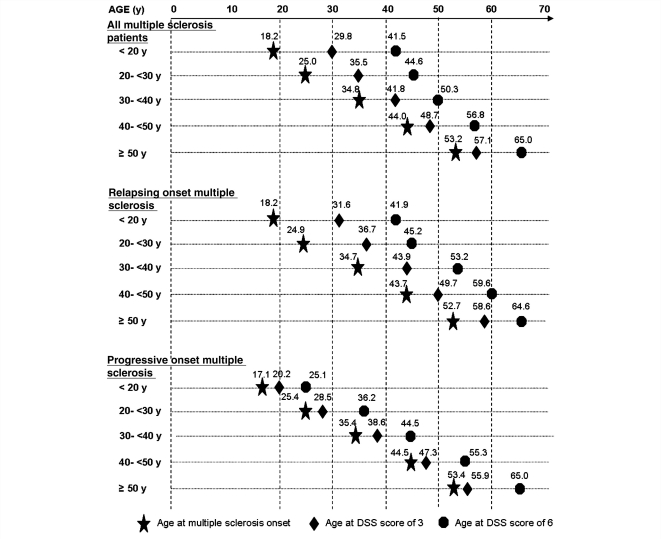
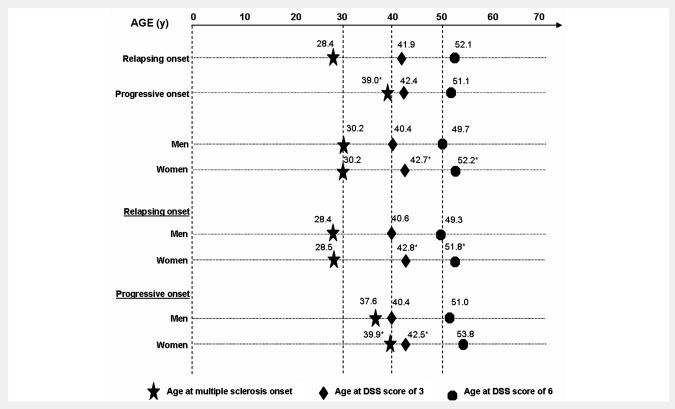
It is well documented that disability accumulation in multiple sclerosis is correlated with axonal injury and that the extent of axonal injury is correlated with the degree of inflammation. However, the interdependence between focal inflammation, diffuse inflammation and neurodegeneration, and their relative contribution to clinical deficits, remains ambiguous. A hypothesis might be that early focal inflammation could be the pivotal event from which all else follows, suggesting the consideration of multiple sclerosis as a two-stage disease. This prompted us to define two phases in the disease course of multiple sclerosis by using two scores on the Kurtzke Disability Status Scale as benchmarks of disability accumulation: an early phase, 'Phase 1', from multiple sclerosis clinical onset to irreversible Disability Status Scale 3 and a late phase, 'Phase 2', from irreversible Disability Status Scale 3 to irreversible Disability Status Scale 6. Outcome was assessed through five parameters: Phase 1 duration, age at Disability Status Scale 3, time to Disability Status Scale 6 from multiple sclerosis onset, Phase 2 duration and age at Disability Status Scale 6. The first three were calculated among all patients, while the last two were computed only among patients who had reached Disability Status Scale 3. The possible influence of early clinical markers on these outcomes was studied using Kaplan-Meier estimates and Cox models. The analysis was performed in the Rennes multiple sclerosis database (2054 patients, accounting for 26,273 patient-years) as a whole, and according to phenotype at onset (1609 relapsing/445 progressive onset). Our results indicated that the disability progression during Phase 2 was independent of that during Phase 1. Indeed, the median Phase 2 duration was nearly identical (from 6 to 9 years) irrespective of Phase 1 duration (<3, 3 to <6, 6 to <10, 10 to <15, >or=15 years) in the whole population, and in both phenotypes. In relapsing onset multiple sclerosis, gender, age at onset, residual deficit after the first relapse and relapses during the first 2 years of multiple sclerosis were found to be independent predictive factors of disability progression, but only during Phase 1. Our findings demonstrate that multiple sclerosis disability progression follows a two-stage process, with a first stage probably dependent on focal inflammation and a second stage probably independent of current focal inflammation. This concept has obvious implications for the future therapeutic strategy in multiple sclerosis.
有大量文献记载,多发性硬化症患者的残疾累积与轴突损伤相关,而轴突损伤的程度又与炎症程度相关。然而,局灶性炎症、弥漫性炎症和神经退行性变之间的相互依赖性,以及它们对临床缺损的相对贡献,仍然不明确。一种假说可能是,早期局灶性炎症可能是所有后续事件的关键事件,这表明可以将多发性硬化症视为一种两阶段疾病。这促使我们使用 Kurtzke 残疾状况量表上的两个分数作为残疾累积的基准,将多发性硬化症的病程定义为两个阶段:早期阶段“阶段 1”,从多发性硬化症临床发病到不可逆的残疾状况量表 3,以及晚期阶段“阶段 2”,从不可逆的残疾状况量表 3 到不可逆的残疾状况量表 6。结果通过五个参数进行评估:阶段 1 的持续时间、达到残疾状况量表 3 时的年龄、从多发性硬化症发病到达到残疾状况量表 6 的时间、阶段 2 的持续时间和达到残疾状况量表 6 时的年龄。前三个参数在所有患者中计算,后两个参数仅在达到残疾状况量表 3 的患者中计算。使用 Kaplan-Meier 估计和 Cox 模型研究了早期临床标志物对这些结果的可能影响。分析在雷恩多发性硬化症数据库(2054 名患者,共计 26273 名患者年)中进行,整体分析,并根据发病时的表型(1609 例复发型/445 例进行性发病)进行分析。结果表明,阶段 2 的残疾进展与阶段 1 的残疾进展无关。事实上,在整个人群中,无论阶段 1 的持续时间如何(<3 年、3-<6 年、6-<10 年、10-<15 年、>=15 年),中位数阶段 2 的持续时间几乎相同(6-9 年),并且在两种表型中均如此。在复发型多发性硬化症中,性别、发病年龄、首次复发后的残留缺陷以及首次复发后 2 年内的复发被认为是残疾进展的独立预测因素,但仅在阶段 1。我们的研究结果表明,多发性硬化症的残疾进展遵循两阶段过程,第一阶段可能依赖于局灶性炎症,第二阶段可能独立于当前的局灶性炎症。这一概念对多发性硬化症未来的治疗策略具有明显的意义。