Department of Oncology, Clinical Sciences, Lund University, Barngatan 2B, Lund, Sweden.
Breast Cancer Res. 2010;12(3):R25. doi: 10.1186/bcr2568. Epub 2010 May 6.
HER2 gene amplification and protein overexpression (HER2+) define a clinically challenging subgroup of breast cancer with variable prognosis and response to therapy. Although gene expression profiling has identified an ERBB2 molecular subtype of breast cancer, it is clear that HER2+ tumors reside in all molecular subtypes and represent a genomically and biologically heterogeneous group, needed to be further characterized in large sample sets.
Genome-wide DNA copy number profiling, using bacterial artificial chromosome (BAC) array comparative genomic hybridization (aCGH), and global gene expression profiling were performed on 200 and 87 HER2+ tumors, respectively. Genomic Identification of Significant Targets in Cancer (GISTIC) was used to identify significant copy number alterations (CNAs) in HER2+ tumors, which were related to a set of 554 non-HER2 amplified (HER2-) breast tumors. High-resolution oligonucleotide aCGH was used to delineate the 17q12-q21 region in high detail.
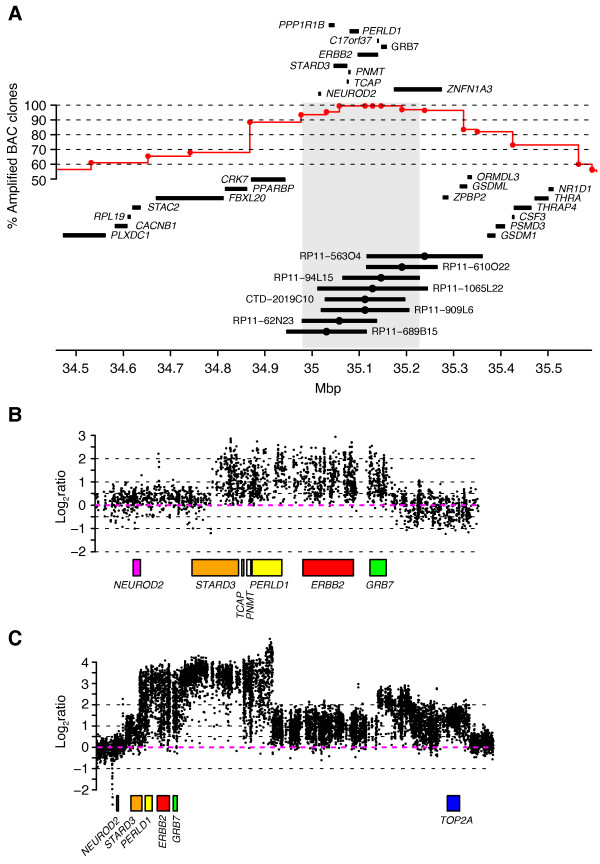
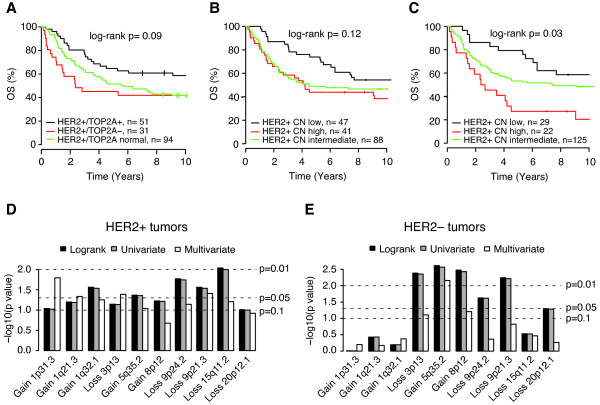
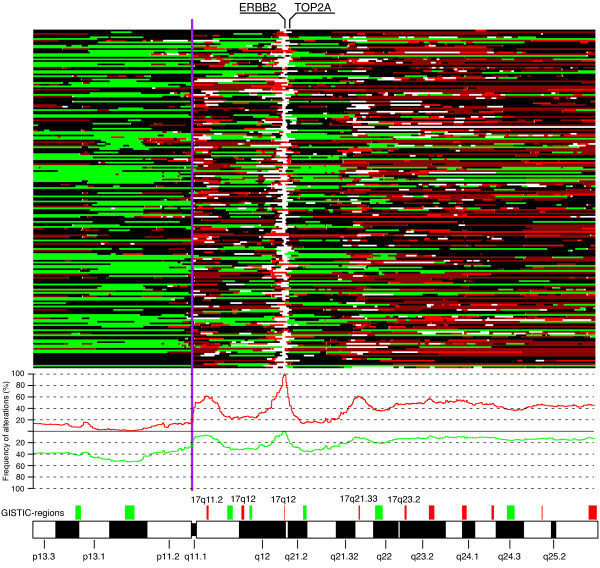
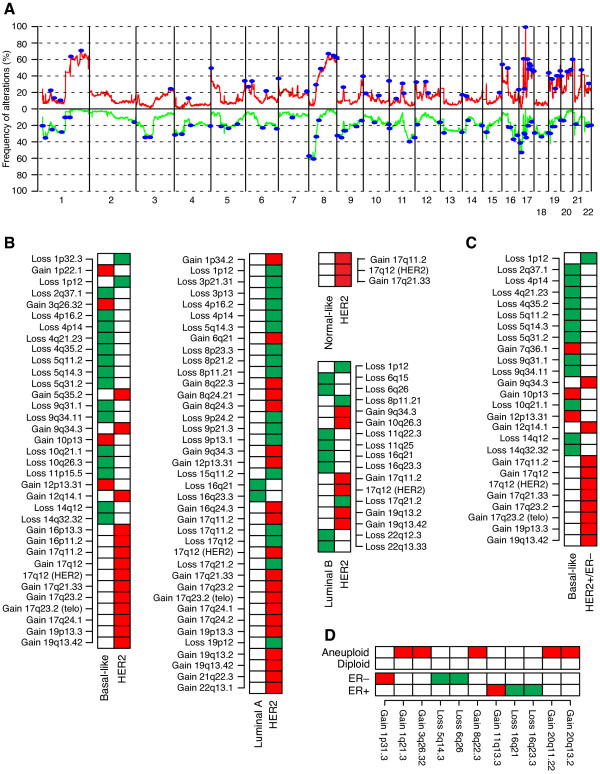
The HER2-amplicon was narrowed to an 85.92 kbp region including the TCAP, PNMT, PERLD1, HER2, C17orf37 and GRB7 genes, and higher HER2 copy numbers indicated worse prognosis. In 31% of HER2+ tumors the amplicon extended to TOP2A, defining a subgroup of HER2+ breast cancer associated with estrogen receptor-positive status and with a trend of better survival than HER2+ breast cancers with deleted (18%) or neutral TOP2A (51%). HER2+ tumors were clearly distinguished from HER2- tumors by the presence of recurrent high-level amplifications and firestorm patterns on chromosome 17q. While there was no significant difference between HER2+ and HER2- tumors regarding the incidence of other recurrent high-level amplifications, differences in the co-amplification pattern were observed, as shown by the almost mutually exclusive occurrence of 8p12, 11q13 and 20q13 amplification in HER2+ tumors. GISTIC analysis identified 117 significant CNAs across all autosomes. Supervised analyses revealed: (1) significant CNAs separating HER2+ tumors stratified by clinical variables, and (2) CNAs separating HER2+ from HER2- tumors.
We have performed a comprehensive survey of CNAs in HER2+ breast tumors, pinpointing significant genomic alterations including both known and potentially novel therapeutic targets. Our analysis sheds further light on the genomically complex and heterogeneous nature of HER2+ tumors in relation to other subgroups of breast cancer.
HER2 基因扩增和蛋白过表达(HER2+)定义了一组具有不同预后和对治疗反应的具有挑战性的乳腺癌临床亚组。虽然基因表达谱分析已经确定了乳腺癌的 ERBB2 分子亚型,但很明显,HER2+肿瘤存在于所有分子亚型中,并且是一组具有基因组和生物学异质性的肿瘤,需要在大样本集中进一步进行特征描述。
使用细菌人工染色体(BAC)阵列比较基因组杂交(aCGH)对 200 例 HER2+肿瘤进行全基因组 DNA 拷贝数分析,并对 87 例 HER2+肿瘤进行全基因组基因表达谱分析。癌症基因组鉴定中的显著靶标(GISTIC)用于鉴定 HER2+肿瘤中的显著拷贝数改变(CNAs),这些改变与一组 554 例非 HER2 扩增(HER2-)乳腺癌肿瘤相关。高分辨率寡核苷酸 aCGH 用于详细描绘 17q12-q21 区域。
HER2 扩增子被缩小到一个 85.92 kbp 区域,包括 TCAP、PNMT、PERLD1、HER2、C17orf37 和 GRB7 基因,并且较高的 HER2 拷贝数预示着更差的预后。在 31%的 HER2+肿瘤中,扩增子延伸到 TOP2A,定义了一组与雌激素受体阳性状态相关的 HER2+乳腺癌亚组,并且与缺失(18%)或中性 TOP2A(51%)的 HER2+乳腺癌相比,具有更好的生存趋势。HER2+肿瘤与 HER2-肿瘤明显不同,因为在染色体 17q 上存在反复出现的高水平扩增和风暴模式。虽然在其他反复出现的高水平扩增的发生率方面,HER2+肿瘤与 HER2-肿瘤之间没有显著差异,但在共扩增模式上观察到差异,这表现为 8p12、11q13 和 20q13 扩增在 HER2+肿瘤中几乎相互排斥。GISTIC 分析在所有常染色体上确定了 117 个显著的 CNA。有监督分析显示:(1)根据临床变量分层的 HER2+肿瘤的显著 CNA,(2)将 HER2+肿瘤与 HER2-肿瘤分开的 CNA。
我们对 HER2+乳腺癌肿瘤中的 CNA 进行了全面调查,确定了包括已知和潜在新治疗靶点在内的显著基因组改变。我们的分析进一步揭示了 HER2+肿瘤与其他乳腺癌亚组相比具有基因组复杂和异质性的性质。