University of South Carolina, Columbia, SC, USA.
Ann Gen Psychiatry. 2010 Jun 2;9:24. doi: 10.1186/1744-859X-9-24.
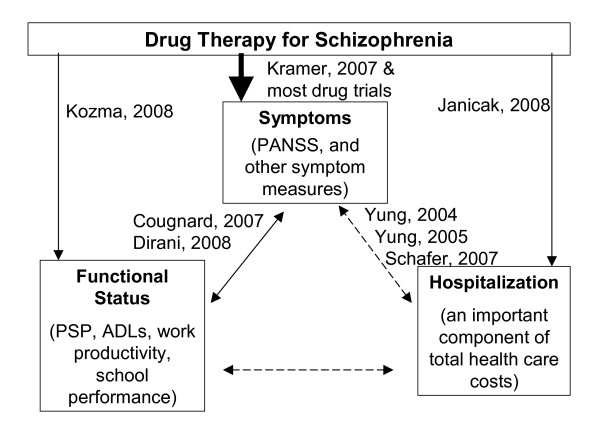
The purpose of this analysis was to evaluate relationships between hospital admission or discharge and scores for symptom or functioning in patients with schizophrenia.
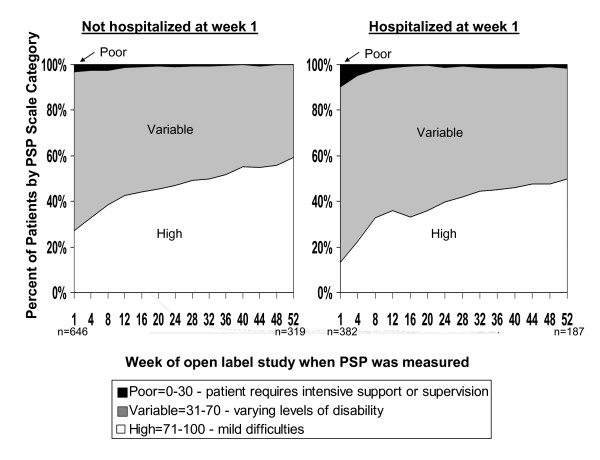
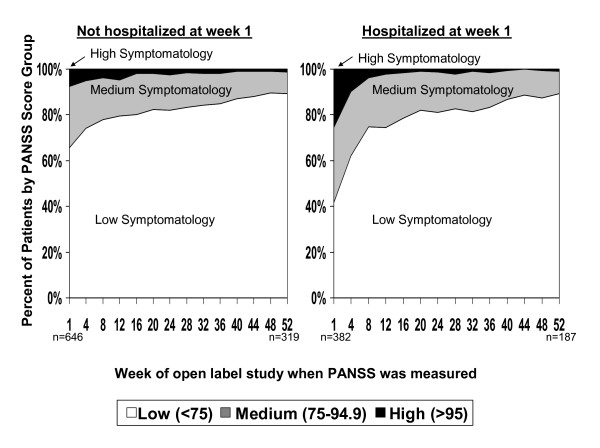
Data were from three 52-week open-label extensions of the double-blind pivotal trials of paliperidone extended-release (ER). Symptoms and patient function were measured every 4 weeks using the Personal and Social Performance (PSP) scale and the Positive and Negative Syndrome Scale (PANSS). The intent-to-treat analysis set was defined as open-label patients who had at least one post-baseline PSP and PANSS measurement. Time until first hospitalization was evaluated using the Cox proportional hazard model with categorical time-dependent measures for the PSP (1 to 30, 31 to 70, 71 to 100) or PANSS (< 75, >/= 75 to < 95, >/= 95), as well as age, gender, schizophrenia duration, and country. Similar analyses were performed for time to discharge.
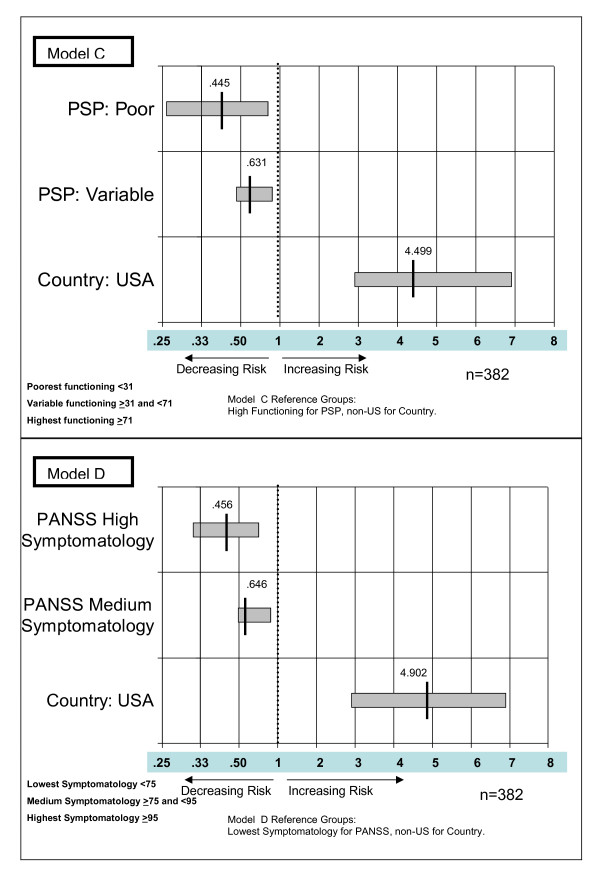
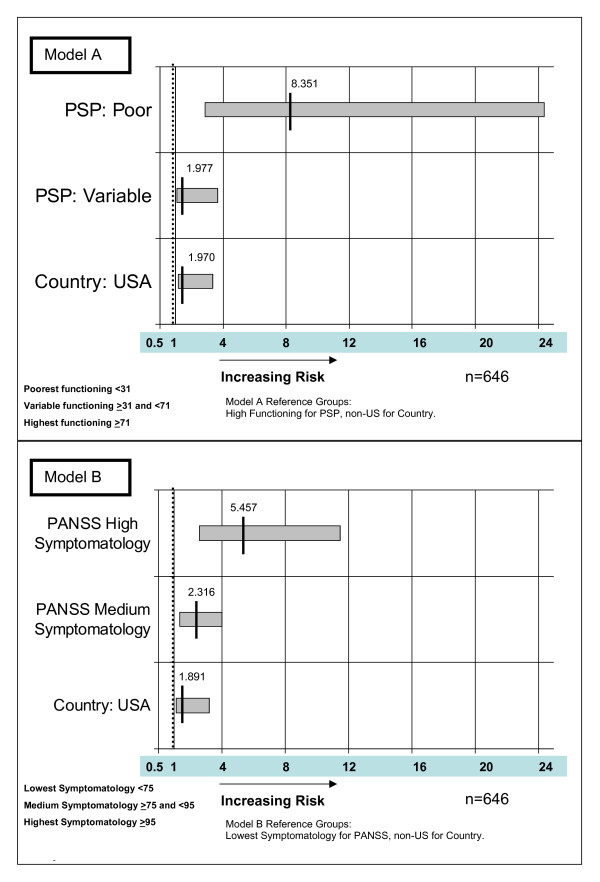
Of the 1,077 enrolled patients, 1,028 (95.5%) met study criteria; of these, 382 (37.2%) were hospitalized at open-label baseline. Compared with patients with PSP >/= 71 group, the hazard for new hospitalization was 8.351 times greater (P = 0.0001) for patients with the poorest functioning (PSP 1 to 30) and 1.977 times greater (P = 0.0295) for patients with PSP of 31-70 compared to the >/= 71 group. The hazard for new hospitalization was 5.457 times greater (P < 0.0001) for patients PANSS >/= 95 and 2.316 times greater (P = 0.0027) for the >/= 75 to < 95 group compared with the < 75 group. For patients hospitalized at baseline, the PANSS >/= 95 patients had a discharge hazard that was 0.456 times lower than for the < 75 patients (P < 0.0001). The hazard for discharge was 0.646 times lower (P = 0.0012) for the PANSS >/= 75 to < 95 group compared with the < 75 group. A patient's country was a significant predictor variable, with US patients being admitted and discharged faster.
Better functioning or being less symptomatic is associated with reduced risk for hospitalization and greater chance for early discharge. Treatments or programs that reduce symptoms or improve function decrease the risk of hospitalization in community patients or increase the chance of discharge for hospitalized patients.
本分析旨在评估精神分裂症患者住院或出院与症状或功能评分之间的关系。
数据来自帕利哌酮缓释片(paliperidone extended-release,paliperidone ER)双盲关键试验的三个 52 周开放标签扩展研究。使用个人和社会功能表现量表(Personal and Social Performance,PSP)和阳性与阴性症状量表(Positive and Negative Syndrome Scale,PANSS)每 4 周测量一次症状和患者功能。意向治疗分析集定义为至少有一次基线后 PSP 和 PANSS 测量的开放标签患者。使用 Cox 比例风险模型评估首次住院时间,使用分类时间依赖的 PSP(1 到 30、31 到 70、71 到 100)或 PANSS(<75、≥75 至 <95、≥95)的类别时间依赖性测量值、年龄、性别、精神分裂症病程和国家作为预测变量。对出院时间进行了类似的分析。
在纳入的 1077 名患者中,有 1028 名(95.5%)符合研究标准;其中,382 名(37.2%)在开放标签基线时住院。与 PSP >/= 71 组相比,功能最差(PSP 1 到 30)的患者新住院的风险高 8.351 倍(P = 0.0001),PSP 为 31-70 的患者高 1.977 倍(P = 0.0295)。与 <75 组相比,PANSS >/= 95 患者新住院的风险高 5.457 倍(P < 0.0001),PANSS >/= 75 至 <95 组患者新住院的风险高 2.316 倍(P = 0.0027)。对于基线住院的患者,PANSS >/= 95 患者的出院风险比 <75 患者低 0.456 倍(P < 0.0001)。与 <75 组相比,PANSS >/= 75 至 <95 组的出院风险低 0.646 倍(P = 0.0012)。患者所在的国家是一个显著的预测变量,美国患者的入院和出院速度更快。
功能更好或症状更少与降低住院风险和增加提前出院的机会相关。减少症状或改善功能的治疗或方案可降低社区患者的住院风险,或增加住院患者出院的机会。