Najar M S, Saldanha C L, Banday K A
Department of Nephrology, Sher-i-Kashmir Institute of Medical Sciences, Soura, Srinagar, J&K, India.
Indian J Nephrol. 2009 Oct;19(4):129-39. doi: 10.4103/0971-4065.59333.
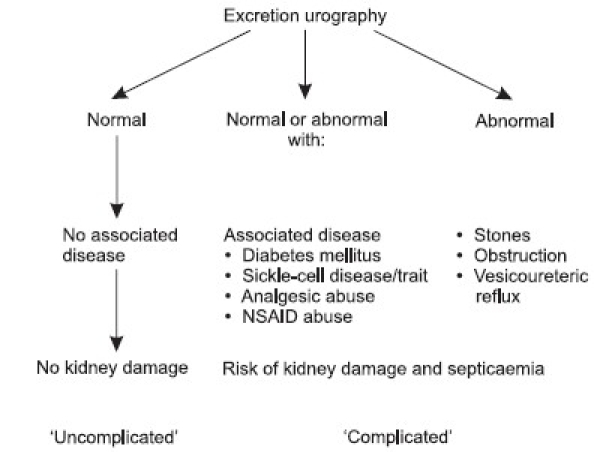
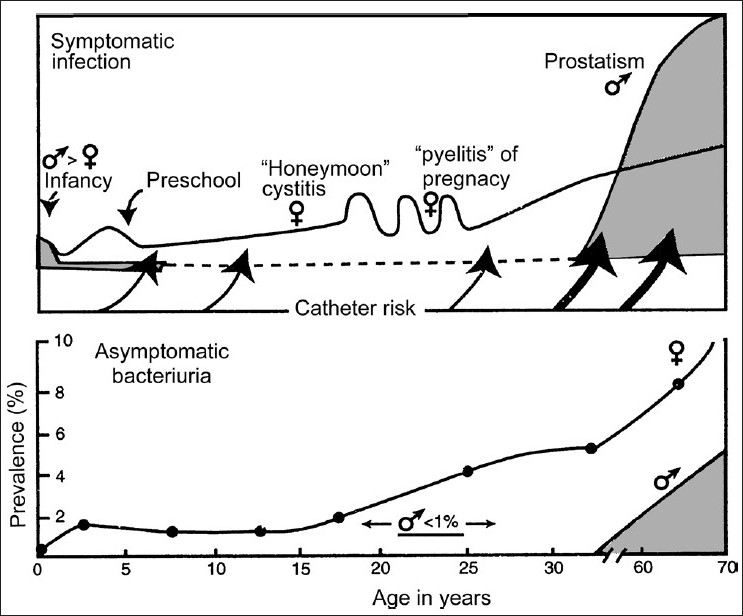
Urinary tract infection (UTI) is the most common infection experienced by humans after respiratory and gastro-intestinal infections, and also the most common cause of both community-acquired and nosocomial infections for patients admitted to hospitals. For better management and prognosis, it is mandatory to know the possible site of infection, whether the infection is uncomplicated or complicated, re-infection or relapse, or treatment failure and its pathogenesis and risk factors. Asymptomatic bacteriuria is common in certain age groups and has different connotations. It needs to be treated and completely cured in pregnant women and preschool children. Reflux nephropathy in children could result in chronic kidney disease; otherwise, urinary tract infections do not play a major role in the pathogenesis of end-stage renal disease. Symptomatic urinary tract infections occur most commonly in women of child-bearing age. Cystitis predominates, but needs to be distinguished from acute urethral syndrome that affects both sexes and has a different management plan than UTIs. The prostatitis symptoms are much more common than bacterial prostatic infections. The treatment needs to be prolonged in bacterial prostatitis and as cure rates are not very high and relapses are common, the classification of prostatitis needs to be understood. The consensus conference convened by National Institute of Health added two more groups of patients, namely, chronic prostatitis/chronic pelvic pain syndrome and asymptomatic inflammatory prostatitis, in addition to acute and chronic bacterial prostatitis. Although white blood cells in urine signify inflammation, they do not always signify UTI. Quantitative cultures of urine provide definitive evidence of UTI. Imaging studies should be done 3-6 weeks after cure of acute infection to identify abnormalities predisposing to infection or renal damage or which may affect management. Treatment of cystitis in women should be a three-day course and if symptoms are prolonged, then a seven day course of antibiotics should be given. Selected group of patients benefits from low-dose prophylactic therapy. Upper urinary tract infection may need in-patient treatment. Treatment of acute prostatitis is 30-day therapy of appropriate antibiotics and for chronic bacterial prostatitis a low dose therapy for 6-12 months may be required. It should be noted that no attempt should be made to eradicate infection unless foreign bodies such as stones and catheters are removed and correctable urological abnormalities are taken care of. Treatment under such circumstances can result only in the emergence of resistant organisms and complicate therapy further.
尿路感染(UTI)是人类继呼吸道和胃肠道感染之后最常见的感染,也是社区获得性感染和医院内感染的最常见原因,这些感染发生在入院患者身上。为了更好地管理和预测病情,必须了解感染的可能部位,感染是单纯性还是复杂性的,是再感染还是复发,或者是治疗失败及其发病机制和危险因素。无症状菌尿在某些年龄组中很常见,并且有不同的含义。在孕妇和学龄前儿童中,它需要得到治疗并完全治愈。儿童反流性肾病可能导致慢性肾病;否则,尿路感染在终末期肾病的发病机制中并不起主要作用。有症状的尿路感染最常发生在育龄妇女中。膀胱炎占主导,但需要与影响两性的急性尿道综合征相区分,后者有与尿路感染不同的管理方案。前列腺炎症状比细菌性前列腺感染更为常见。细菌性前列腺炎的治疗需要延长疗程,而且由于治愈率不是很高且复发很常见,需要了解前列腺炎的分类。美国国立卫生研究院召开的共识会议除了急性和慢性细菌性前列腺炎外,又增加了两组患者,即慢性前列腺炎/慢性盆腔疼痛综合征和无症状性炎性前列腺炎。虽然尿中的白细胞表示炎症,但它们并不总是意味着存在尿路感染。尿液的定量培养提供了尿路感染的确切证据。急性感染治愈后3至6周应进行影像学检查,以确定易导致感染或肾损害或可能影响治疗的异常情况。女性膀胱炎的治疗疗程应为三天,如果症状持续,则应给予七天的抗生素疗程。部分选定的患者从低剂量预防性治疗中受益。上尿路感染可能需要住院治疗。急性前列腺炎的治疗是使用适当的抗生素进行30天治疗,而慢性细菌性前列腺炎可能需要进行6至12个月的低剂量治疗。需要注意的是,除非取出结石和导管等异物并处理可纠正的泌尿系统异常情况,否则不应试图根除感染。在这种情况下进行治疗只会导致耐药菌的出现,并使治疗进一步复杂化。