Department of Public Health, University of Otago, Wellington, New Zealand.
BMC Public Health. 2010 Jun 11;10:332. doi: 10.1186/1471-2458-10-332.
The new International Health Regulations (IHR) require World Health Organization (WHO) member states to assess their core capacity for surveillance. Such reviews also have the potential to identify important surveillance gaps, improve the organisation of disparate surveillance systems and to focus attention on upstream hazards, determinants and interventions.
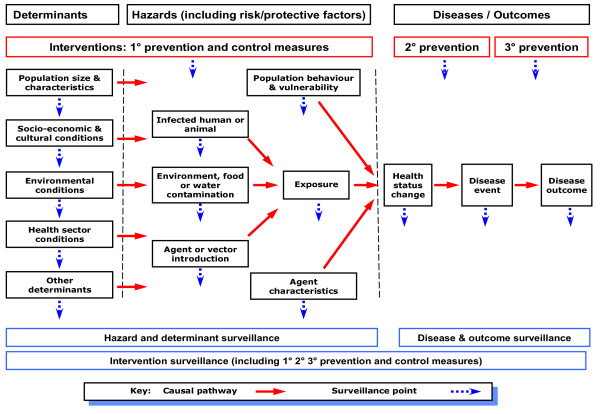
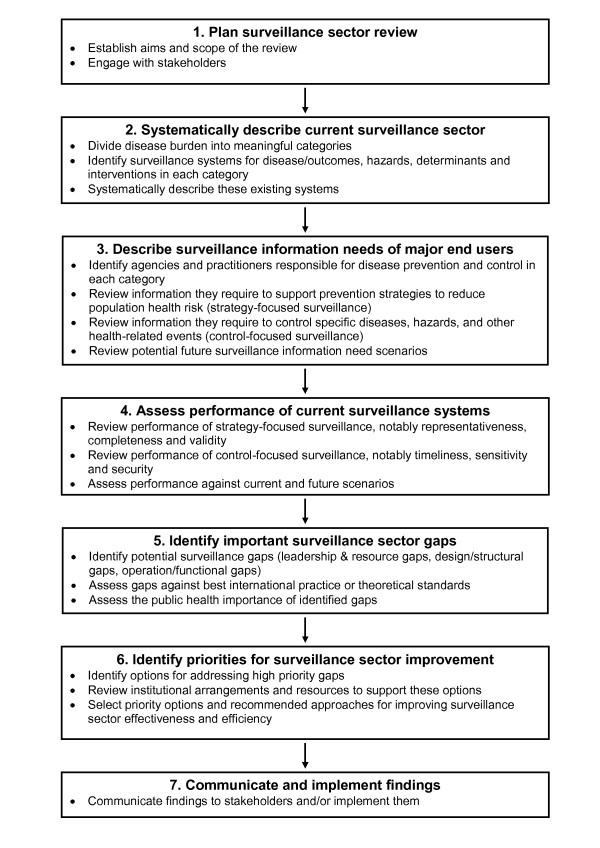
We developed a surveillance sector review method for evaluating all of the surveillance systems and related activities across a sector, in this case those concerned with infectious diseases in New Zealand. The first stage was a systematic description of these surveillance systems using a newly developed framework and classification system. Key informant interviews were conducted to validate the available information on the systems identified.
We identified 91 surveillance systems and related activities in the 12 coherent categories of infectious diseases examined. The majority (n = 40 or 44%) of these were disease surveillance systems. They covered all categories, particularly for more severe outcomes including those resulting in death or hospitalisations. Except for some notifiable diseases and influenza, surveillance of less severe, but important infectious diseases occurring in the community was largely absent. There were 31 systems (34%) for surveillance of upstream infectious disease hazards, including risk and protective factors. This area tended to have many potential gaps and lack integration, partly because such systems were operated by a range of different agencies, often outside the health sector. There were fewer surveillance systems for determinants, including population size and characteristics (n = 9), and interventions (n = 11).
It was possible to create and populate a workable framework for describing all the infectious diseases surveillance systems and related activities in a single developed country and to identify potential surveillance sector gaps. This is the first stage in a review process that will lead to identification of priorities for surveillance sector development.
新的《国际卫生条例(IHR)》要求世界卫生组织(WHO)成员国评估其监测核心能力。此类审查还有可能发现重要的监测差距,改善不同监测系统的组织,并将重点放在上游危害、决定因素和干预措施上。
我们开发了一种监测部门审查方法,用于评估一个部门(在此情况下为新西兰传染病部门)的所有监测系统和相关活动。第一阶段是使用新开发的框架和分类系统对这些监测系统进行系统描述。对确定的系统进行了关键信息提供者访谈,以验证现有信息的准确性。
我们在审查的 12 个连贯传染病类别中发现了 91 个监测系统和相关活动。其中大多数(n=40 或 44%)是疾病监测系统。它们涵盖了所有类别,特别是针对更严重的结果,包括导致死亡或住院的结果。除了一些法定传染病和流感外,对在社区中发生的不太严重但重要的传染病的监测基本上不存在。有 31 个系统(34%)用于监测上游传染病危害,包括风险和保护因素。这一领域往往存在许多潜在的差距,并且缺乏整合,部分原因是这些系统由一系列不同的机构操作,通常不在卫生部门内。用于确定因素,包括人口规模和特征(n=9)和干预措施(n=11)的监测系统较少。
有可能为一个发达国家创建和填充一个可行的框架,用于描述所有传染病监测系统和相关活动,并确定潜在的监测部门差距。这是审查过程的第一阶段,将导致确定监测部门发展的优先事项。