Institute of General Practice and Health Services Research, University of Zurich, Zurich, Switzerland.
Cardiovasc Diabetol. 2010 Jun 15;9:23. doi: 10.1186/1475-2840-9-23.
Diabetes is a major challenge for the health care system and especially for the primary care provider. The Chronic Care Model represents an evidence-based framework for the care for chronically ill. An increasing number of studies showed that implementing elements of the Chronic Care Model improves patient relevant outcomes and process parameters. However, most of these findings have been performed in settings different from the Swiss health care system which is dominated by single handed practices.
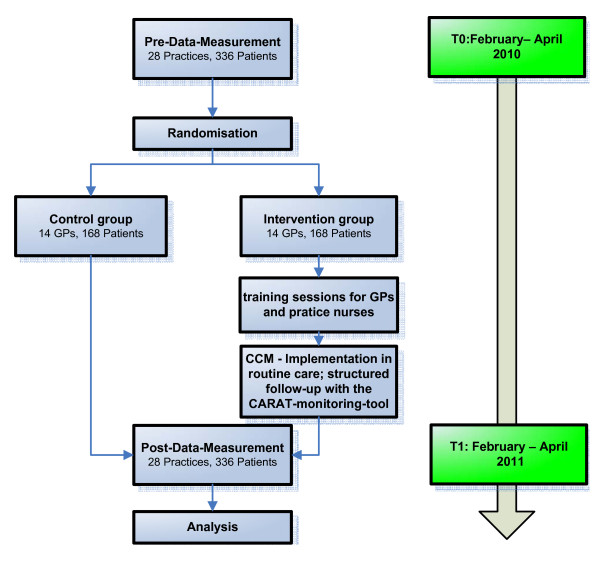
METHODS/DESIGN: CARAT is a cluster randomized controlled trial with general practitioners as the unit of randomization (trial registration: ISRCTN05947538). The study challenges the hypothesis that implementing several elements of the Chronic Care Model via a specially trained practice nurse improves the HbA1c level of diabetes type II patients significantly after one year (primary outcome). Furthermore, we assume that the intervention increases the proportion of patients who achieve the recommended targets regarding blood pressure (<130/80), HbA1c (=<6.5%) and low-density lipoprotein-cholesterol (<2.6 mmol/l), increases patients' quality of life (SF-36) and several evidence-based quality indicators for diabetes care. These improvements in care will be experienced by the patients (PACIC-5A) as well as by the practice team (ACIC). According to the power calculation, 28 general practitioners will be randomized either to the intervention group or to the control group. Each general practitioner will include 12 patients suffering from diabetes type II. In the intervention group the general practitioner as well as the practice nurse will be trained to perform care for diabetes patients according to the Chronic Care Model in teamwork. In the control group no intervention will be applied at all and patients will be treated as usual. Measurements (pre-data-collection) will take place in months II-IV, starting in February 2010. Follow-up data will be collected after 1 year.
This study challenges the hypothesis that the Chronic Care Model can be easily implemented by a practice nurse focused approach. If our results will confirm this hypothesis the suggestion arises whether this approach should be implemented in other chronic diseases and multimorbid patients and how to redesign care in Switzerland.
糖尿病是医疗保健系统面临的主要挑战,尤其是对初级保健提供者而言。慢性病照护模式是一种针对慢性病患者的循证护理框架。越来越多的研究表明,实施慢性病照护模式的各项元素可以改善患者相关的结局和流程参数。然而,这些发现大多是在与瑞士医疗保健系统不同的环境中进行的,瑞士的医疗保健系统主要由单人执业医师主导。
方法/设计:CARAT 是一项针对全科医生的群组随机对照试验(试验注册:ISRCTN05947538)。该研究对以下假设提出了挑战,即通过专门培训的执业护士实施慢性病照护模式的几个元素,可以在一年后显著改善 II 型糖尿病患者的糖化血红蛋白(HbA1c)水平(主要结局)。此外,我们假设该干预措施可以提高达到血压(<130/80)、HbA1c(<6.5%)和低密度脂蛋白胆固醇(<2.6 mmol/l)推荐目标的患者比例,提高患者的生活质量(SF-36)和几项循证糖尿病护理质量指标。患者(PACIC-5A)和执业团队(ACIC)都将体验到这些护理的改善。根据计算的功效,将有 28 名全科医生被随机分配到干预组或对照组。每位全科医生将纳入 12 名 II 型糖尿病患者。在干预组中,全科医生和执业护士将接受培训,以团队合作的方式根据慢性病照护模式为糖尿病患者提供护理。在对照组中,将不进行任何干预,患者将按常规治疗。测量(预数据收集)将在 2010 年 2 月开始的第 II-IV 个月进行。随访数据将在 1 年后收集。
本研究对以下假设提出了挑战,即慢性病照护模式可以通过以执业护士为重点的方法轻松实施。如果我们的结果证实了这一假设,那么就会出现这样的建议,即在其他慢性病和多种疾病患者中是否应实施这种方法,以及如何重新设计瑞士的护理。