Clinic of Anesthesiology and Intensive Care Medicine, Charité University Medicine, Campus Virchow-Klinikum, Augustenburger Platz 1, 13353 Berlin, Germany.
Crit Care. 2010;14(3):R119. doi: 10.1186/cc9074. Epub 2010 Jun 18.
Non-excitable muscle membrane indicates critical illness myopathy (CIM) during early critical illness. We investigated predisposing risk factors for non-excitable muscle membrane at onset of critical illness.
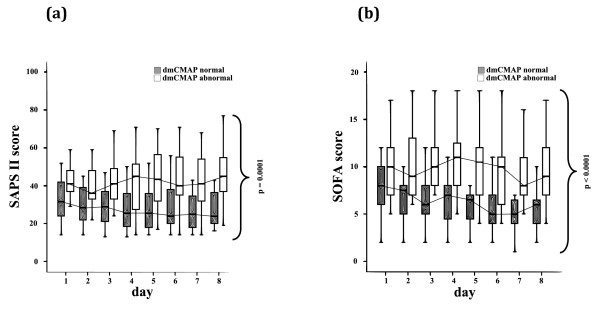
We performed sequential measurements of muscle membrane excitability after direct muscle stimulation (dmCMAP) in 40 intensive care unit (ICU) patients selected upon a simplified acute physiology (SAPS-II) score >OR= 20 on 3 successive days within 1 week after ICU admission. We then investigated predisposing risk factors, including the insulin-like growth factor (IGF)-system, inflammatory, metabolic and hemodynamic parameters, as well as suspected medical treatment prior to first occurrence of abnormal dmCMAP. Nonparametric analysis of two-factorial longitudinal data and multivariate analysis were used for statistical analysis.
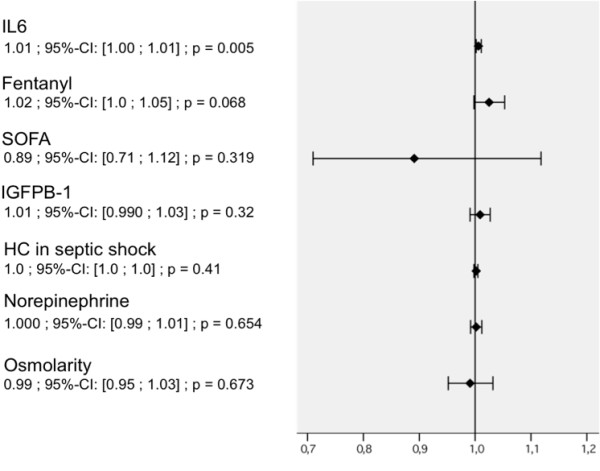
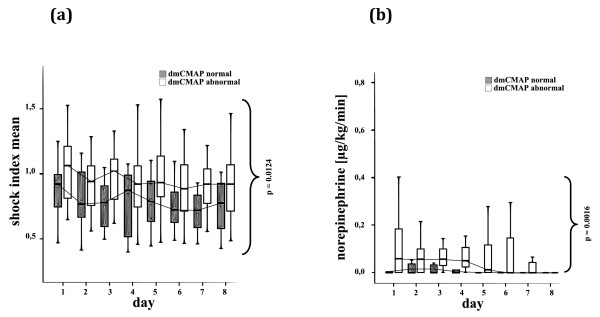
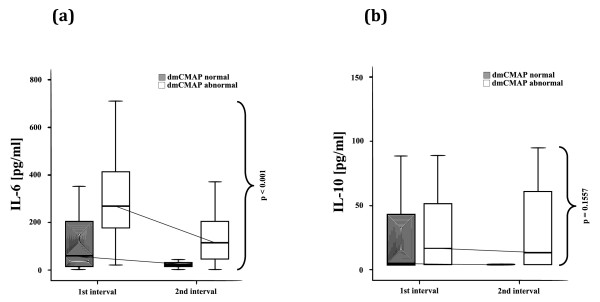
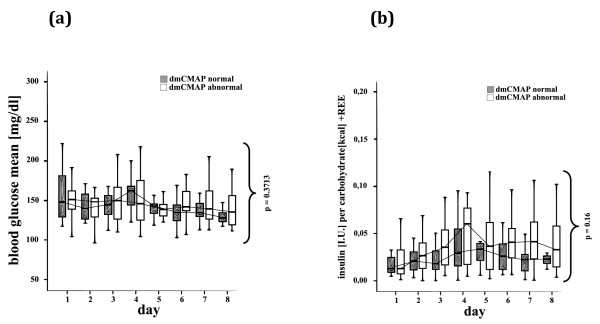
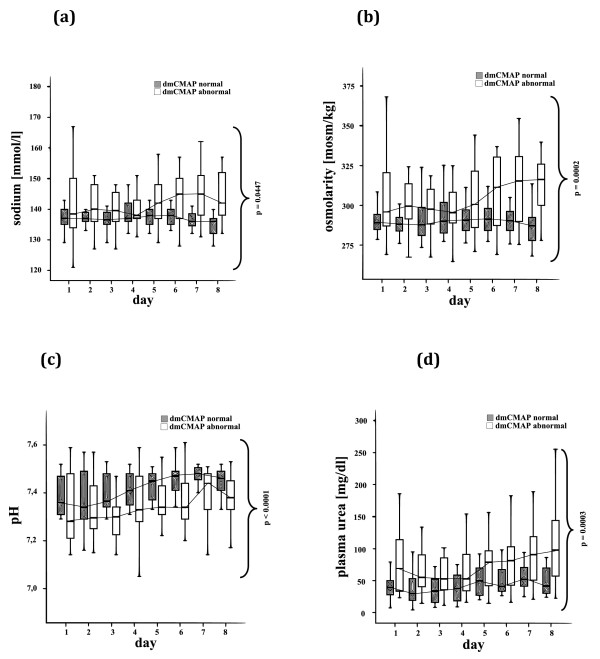
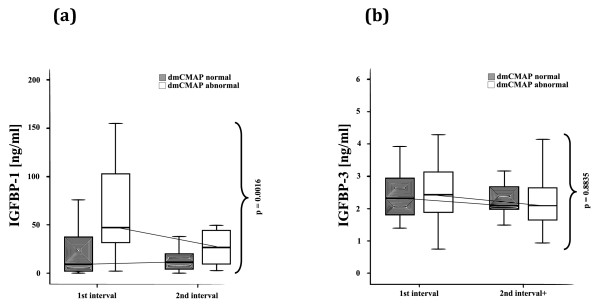
22 patients showed abnormal muscle membrane excitability during direct muscle stimulation within 7 (5 to 9.25) days after ICU admission. Significant risk factors for the development of impaired muscle membrane excitability in univariate analysis included inflammation, disease severity, catecholamine and sedation requirements, as well as IGF binding protein-1 (IGFBP-I), but did not include either adjunctive hydrocortisone treatment in septic shock, nor administration of neuromuscular blocking agents or aminoglycosides. In multivariate Cox regression analysis, interleukin-6 remained the significant risk factor for the development of impaired muscle membrane excitability (HR 1.006, 95%-CI (1.002 to 1.011), P = 0.002).
Systemic inflammation during early critical illness was found to be the main risk factor for development of CIM during early critical illness. Inflammation-induced impairment of growth-factor mediated insulin sensitivity may be involved in the development of CIM.
非兴奋肌膜在疾病早期提示危重病肌病(CIM)。我们研究了疾病早期发生非兴奋肌膜的易感危险因素。
我们对 40 名 ICU 患者连续进行了 3 天的简化急性生理学评分(SAPS-II)>20 分,在 ICU 入院后 1 周内,每天进行 3 次直接肌肉刺激(dmCMAP)后,对肌膜兴奋性进行了连续测量。然后,我们调查了易感危险因素,包括胰岛素样生长因子(IGF)系统、炎症、代谢和血液动力学参数,以及可疑的医学治疗,这些都是在首次出现异常 dmCMAP 之前。我们采用两因素纵向数据的非参数分析和多变量分析进行统计学分析。
22 例患者在 ICU 入院后 7(5 至 9.25)天内直接肌肉刺激时出现异常肌膜兴奋性。单因素分析中,炎症、疾病严重程度、儿茶酚胺和镇静要求,以及 IGF 结合蛋白-1(IGFBP-1)是肌肉膜兴奋性受损的显著危险因素,但脓毒症休克时辅助应用皮质醇治疗,或使用神经肌肉阻滞剂或氨基糖苷类药物均不是其危险因素。多变量 Cox 回归分析中,白细胞介素-6 仍然是肌肉膜兴奋性受损的显著危险因素(HR 1.006,95%-CI(1.002 至 1.011),P=0.002)。
早期危重病期间的全身炎症被认为是早期危重病中 CIM 发展的主要危险因素。炎症诱导的生长因子介导的胰岛素敏感性受损可能与 CIM 的发生有关。