Department of Medicine RMH/WH, The University of Melbourne, 4th Floor Clinical Sciences Building, The Royal Melbourne Hospital, Parkville, Victoria 3050, Australia.
Malar J. 2010 Jun 24;9:181. doi: 10.1186/1475-2875-9-181.
Artemisinin derivatives have been used for malaria treatment in Vietnam since 1989. Reported malaria cases have decreased from 1,672,000 with 4,650 deaths in 1991, to 91,635 with 43 deaths in 2006. Current national guidelines recommend artemisinin-based combination therapy (ACT), although artesunate is still available as monotherapy through the private sector. Recent reports suggest that effectiveness of ACT and artesunate monotherapy has declined in western Cambodia. This study examined Plasmodium falciparum resistance patterns over 10 years in southwest Vietnam in infected patients treated with artemisinin compounds.
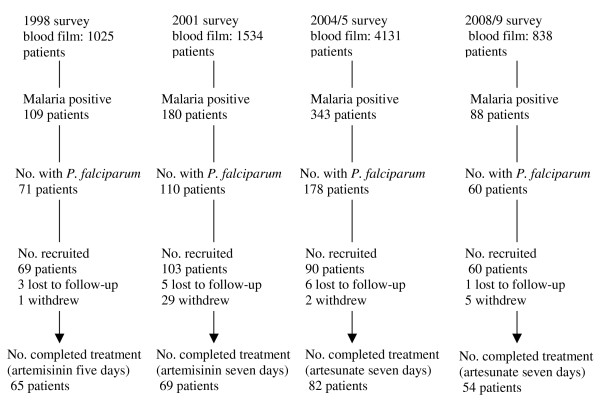
The study was conducted in two communes in Phuoc Long district, Binh Phuoc province, 100 km west of the Cambodian border. This was chosen as a likely site for emerging artemisinin resistance because of the high prevalence of P. falciparum malaria, and the length of time that artemisinin had been in use. In vivo and in vitro monitoring of P. falciparum susceptibility to anti-malarial drugs was conducted in 1998, 2001, 2004/5, and 2008/9. Patients with confirmed P. falciparum malaria received therapy with 5 or 7 days of artemisinin (1998 and 2001 respectively) or 7 days of artesunate
In the four surveys, 270 patients were recruited and treated. The mean parasite clearance times differed between 1998, 2001 and 2004/5 (1.8, 2.3 and 2.1 days, P < 0.01) but not between 1998 and 2008/2009. The mean parasite clearance times were correlated with parasite density at day 0 (r = 0.4; P < 0.001). Treatment failure rates after PCR adjustment were 13.8%, 2.9%, 1.2%, and 0% respectively. Susceptibility of P. falciparum to artemisinin in in vitro tests was stable during the period, except for a rise in EC90 and EC99 in 2001.
This study showed stable levels of P. falciparum sensitivity to artemisinin compounds in the two sites over a ten-year period. The introduction of ACT in this area in 2003 may have protected against the development of artemisinin resistance. Adherence to the latest WHO and Vietnamese guidelines, which recommend ACT as first-line therapy in all malarious areas, and continued monitoring along the Vietnam-Cambodia border will be essential to prevent the spread of artemisinin resistance in Vietnam.
自 1989 年以来,青蒿素衍生物一直在越南用于治疗疟疾。报告的疟疾病例已从 1991 年的 1672000 例和 4650 例死亡下降到 2006 年的 91635 例和 43 例死亡。目前的国家指南建议使用青蒿素为基础的联合治疗(ACT),尽管青蒿琥酯仍可通过私营部门作为单一疗法使用。最近的报告表明,柬埔寨西部青蒿琥酯单药治疗和 ACT 的疗效有所下降。本研究在越南西南部的两个公社(富隆区,平定省)检测了 10 年来感染接受青蒿素类化合物治疗的疟原虫耐药模式。
该研究在柬埔寨边境以西 100 公里的平定省富隆区的两个公社进行。由于恶性疟原虫疟疾的高流行率以及青蒿素的使用时间,选择该地区作为青蒿素耐药性出现的可能地点。1998 年、2001 年、2004/5 年和 2008/9 年对疟原虫对抗疟药物的敏感性进行了体内和体外监测。确诊为恶性疟原虫疟疾的患者接受了 5 天或 7 天的青蒿素(分别为 1998 年和 2001 年)或 7 天的青蒿琥酯治疗。
在四项调查中,共招募和治疗了 270 名患者。寄生虫清除时间在 1998 年、2001 年和 2004/5 年之间存在差异(1.8、2.3 和 2.1 天,P < 0.01),但 1998 年和 2008/2009 年之间没有差异。寄生虫清除时间与第 0 天的寄生虫密度相关(r = 0.4;P < 0.001)。PCR 调整后的治疗失败率分别为 13.8%、2.9%、1.2%和 0%。在这一期间,除 2001 年 EC90 和 EC99 升高外,疟原虫对青蒿素的体外敏感性保持稳定。
本研究显示,在十年期间,两个地点的恶性疟原虫对青蒿素类化合物的敏感性保持稳定。2003 年在该地区引入 ACT 可能有助于防止青蒿素耐药性的发展。遵循最新的世界卫生组织和越南指南,建议在所有疟疾地区将 ACT 作为一线治疗药物,以及沿越南-柬埔寨边境继续监测,对于防止越南青蒿素耐药性的传播至关重要。