Endocrine Cancer Group, Edinburgh Cancer Research Centre, Edinburgh University, Carrington Crescent, Edinburgh EH4 2XU, UK.
Breast Cancer Res. 2010;12(4):R47. doi: 10.1186/bcr2604. Epub 2010 Jul 8.
Patients with early-stage breast cancer, treated with endocrine therapy, have approximately 90% 5-year disease-free survival. However, for patients at higher risk of relapse despite endocrine therapy, additional adjuvant therapy, such as chemotherapy, may be indicated. The challenge is to prospectively identify such patients. The Mammostrat® test uses five immunohistochemical markers to stratify patients on tamoxifen therapy into risk groups to inform treatment decisions. We tested the efficacy of this panel in a mixed population of cases treated in a single center with breast-conserving surgery and long-term follow-up.
Tissue microarrays from a consecutive series (1981 to 1998) of 1,812 women managed by wide local excision and postoperative radiotherapy were collected following appropriate ethical review. Of 1,390 cases stained, 197 received no adjuvant hormonal or chemotherapy, 1,044 received tamoxifen only, and 149 received a combination of hormonal therapy and chemotherapy. Median age at diagnosis was 57, 71% were postmenopausal, 23.9% were node-positive and median tumor size was 1.5 cm. Samples were stained using triplicate 0.6 mm2 tissue microarray cores, and positivity for p53, HTF9C, CEACAM5, NDRG1 and SLC7A5 was assessed. Each case was assigned a Mammostrat risk score, and distant recurrence-free survival (DRFS), relapse-free survival (RFS) and overall survival (OS) were analyzed by marker positivity and risk score.
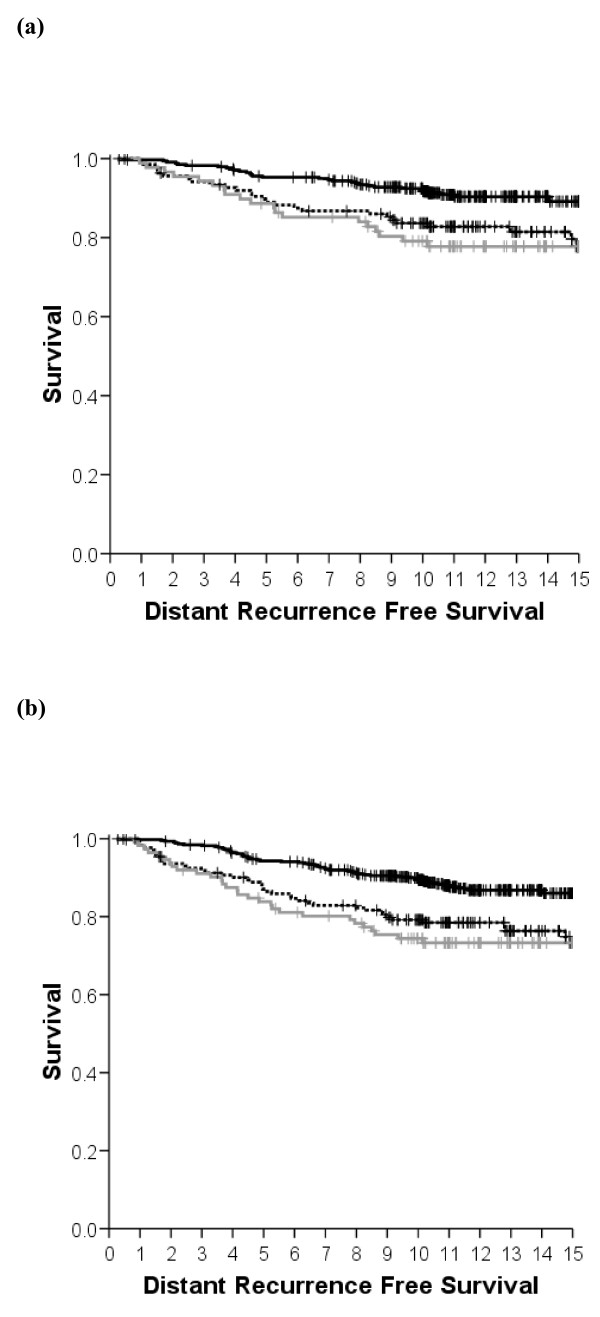
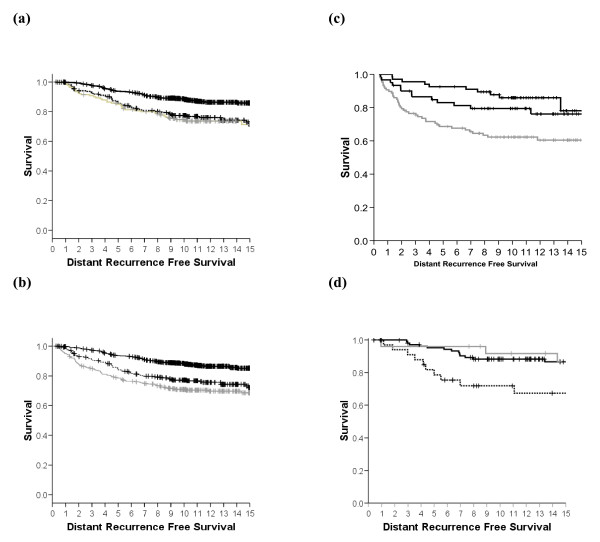
Increased Mammostrat scores were significantly associated with reduced DRFS, RFS and OS in estrogen receptor (ER)-positive breast cancer (P < 0.00001). In multivariate analyses the risk score was independent of conventional risk factors for DRFS, RFS and OS (P < 0.05). In node-negative, tamoxifen-treated patients, 10-year recurrence rates were 7.6 ± 1.5% in the low-risk group versus 20.0 ± 4.4% in the high-risk group. Further, exploratory analyses revealed associations with outcome in both ER-negative and untreated patients.
This is the fifth independent study providing evidence that Mammostrat can act as an independent prognostic tool for ER-positive, tamoxifen-treated breast cancer. In addition, this study revealed for the first time a possible association with outcome regardless of node status and ER-negative tumors. When viewed in the context of previous results, these data provide further support for this antibody panel as an aid to patient management in early-stage breast cancer.
接受内分泌治疗的早期乳腺癌患者,5 年无病生存率约为 90%。然而,对于内分泌治疗后仍有较高复发风险的患者,可能需要辅助化疗等其他治疗。问题在于如何前瞻性地识别这些患者。Mammostrat®检测使用 5 种免疫组化标志物,将接受他莫昔芬治疗的患者分为风险组,以告知治疗决策。我们在一家中心接受保乳手术和长期随访治疗的混合病例系列中测试了该面板的疗效。
在适当的伦理审查后,收集了 1981 年至 1998 年连续系列(1812 例)接受广泛局部切除和术后放疗的女性的组织微阵列。在 1390 例可染色的病例中,197 例未接受辅助激素或化疗,1044 例仅接受他莫昔芬治疗,149 例接受激素联合化疗。中位诊断年龄为 57 岁,71%绝经后,23.9%淋巴结阳性,中位肿瘤大小为 1.5 厘米。使用三重复制 0.6 毫米 2 组织微阵列核心进行样品染色,并评估 p53、HTF9C、CEACAM5、NDRG1 和 SLC7A5 的阳性率。每个病例均被分配 Mammostrat 风险评分,并根据标记物阳性率和风险评分分析远处无复发生存率(DRFS)、无复发生存率(RFS)和总生存(OS)。
在雌激素受体(ER)阳性乳腺癌中,Mammostrat 评分升高与 DRFS、RFS 和 OS 降低显著相关(P<0.00001)。在多变量分析中,风险评分独立于 DRFS、RFS 和 OS 的传统危险因素(P<0.05)。在淋巴结阴性、接受他莫昔芬治疗的患者中,低危组 10 年复发率为 7.6±1.5%,高危组为 20.0±4.4%。此外,探索性分析显示,该评分与 ER 阴性和未治疗患者的预后相关。
这是第五项独立研究,证明 Mammostrat 可作为 ER 阳性、接受他莫昔芬治疗的乳腺癌的独立预后工具。此外,本研究首次揭示了与结局的关联,无论淋巴结状态和 ER 阴性肿瘤如何。结合以前的结果来看,这些数据进一步支持该抗体面板作为早期乳腺癌患者管理的辅助工具。