Department of Intensive Care Medicine, The Queen Elizabeth Hospital, 28 Woodville Road, Woodville, South Australia 5011, Australia.
Crit Care. 2010;14(4):R134. doi: 10.1186/cc9182. Epub 2010 Jul 13.
Current low (stress) dose corticosteroid regimens may have therapeutic advantage in severe sepsis and septic shock despite conflicting results from two landmark randomised controlled trials (RCT). We systematically reviewed the efficacy of corticosteroid therapy in severe sepsis and septic shock.
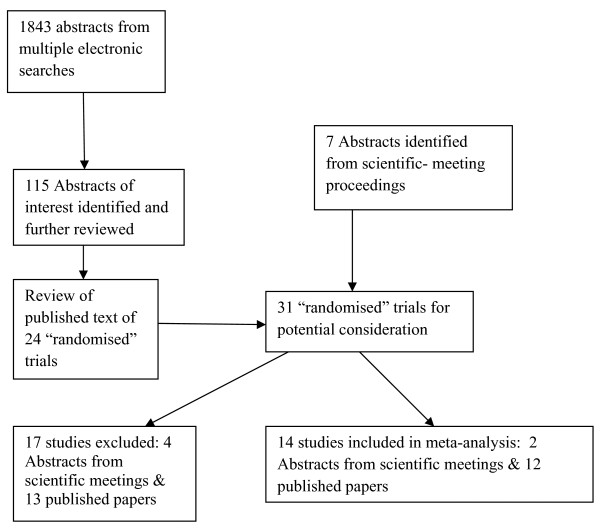
RCTs were identified (1950-September 2008) by multiple data-base electronic search (MEDLINE via OVID, OVID PreMedline, OVID Embase, Cochrane Central Register of Controlled trials, Cochrane database of systematic reviews, Health Technology Assessment Database and Database of Abstracts of Reviews of Effects) and hand search of references, reviews and scientific society proceedings. Three investigators independently assessed trial inclusion and data extraction into standardised forms; differences resolved by consensus.
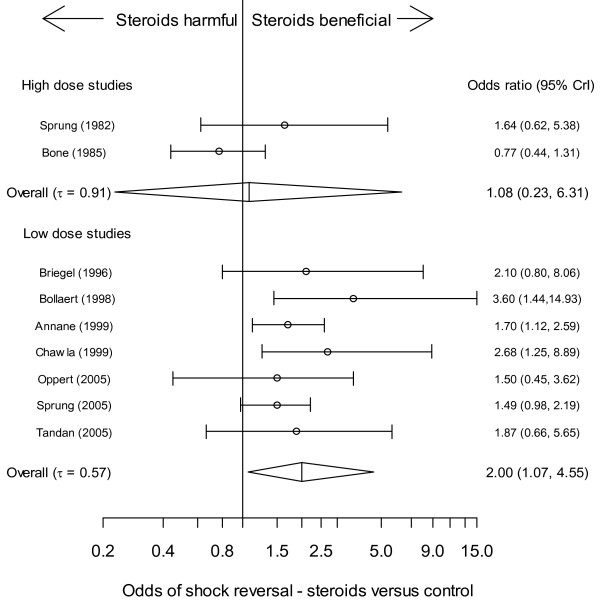
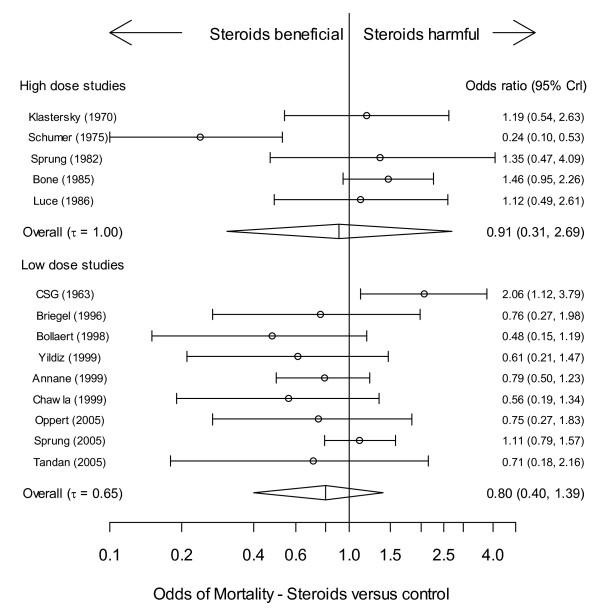
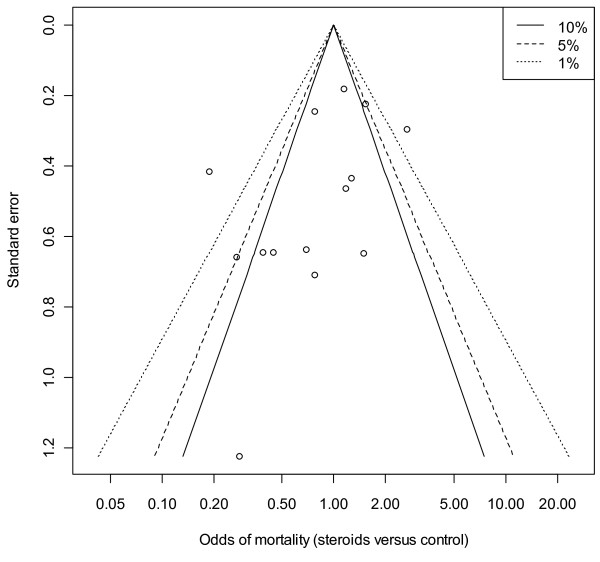
Corticosteroid efficacy, compared with control, for hospital-mortality, proportion of patients experiencing shock-resolution, and infective and non-infective complications was assessed using Bayesian random-effects models; expressed as odds ratio (OR, (95% credible-interval)). Bayesian outcome probabilities were calculated as the probability (P) that OR ≥1. Fourteen RCTs were identified. High-dose (>1000 mg hydrocortisone (equivalent) per day) corticosteroid trials were associated with a null (n = 5; OR 0.91(0.31-1.25)) or higher (n = 4, OR 1.46(0.73-2.16), outlier excluded) mortality probability (P = 42.0% and 89.3%, respectively). Low-dose trials (<1000 mg hydrocortisone per day) were associated with a lower (n = 9, OR 0.80(0.40-1.39); n = 8 OR 0.71(0.37-1.10), outlier excluded) mortality probability (20.4% and 5.8%, respectively). OR for shock-resolution was increased in the low dose trials (n = 7; OR 1.20(1.07-4.55); P = 98.2%). Patient responsiveness to corticotrophin stimulation was non-determinant. A high probability of risk-related treatment efficacy (decrease in log-odds mortality with increased control arm risk) was identified by metaregression in the low dose trials (n = 9, slope coefficient -0.49(-1.14, 0.27); P = 92.2%). Odds of complications were not increased with corticosteroids.
Although a null effect for mortality treatment efficacy of low dose corticosteroid therapy in severe sepsis and septic shock was not excluded, there remained a high probability of treatment efficacy, more so with outlier exclusion. Similarly, although a null effect was not excluded, advantageous effects of low dose steroids had a high probability of dependence upon patient underlying risk. Low dose steroid efficacy was not demonstrated in corticotrophin non-responders. Further large-scale trials appear mandated.
目前的低(应激)剂量皮质类固醇治疗方案在严重脓毒症和败血症性休克中可能具有治疗优势,尽管两项具有里程碑意义的随机对照试验(RCT)得出了相互矛盾的结果。我们系统地回顾了皮质类固醇治疗严重脓毒症和败血症性休克的疗效。
通过多个数据库电子搜索(通过 OVID 的 MEDLINE、OVID PreMedline、OVID Embase、Cochrane 对照试验注册中心、Cochrane 系统评价数据库、卫生技术评估数据库和效果摘要数据库)和手工搜索参考文献、综述和科学学会会议,确定了 RCT(1950 年-2008 年 9 月)。三位研究人员独立评估了试验纳入标准和数据提取到标准表格中;通过共识解决差异。
使用贝叶斯随机效应模型评估了与对照组相比,皮质激素治疗的住院死亡率、休克缓解患者比例以及感染性和非感染性并发症的疗效;表示为比值比(OR,(95%可信区间))。贝叶斯结局概率被计算为 OR≥1 的概率(P)。确定了 14 项 RCT。高剂量(>1000mg 氢化可的松(等效物)/天)皮质类固醇试验与死亡率的零(n=5;OR 0.91(0.31-1.25))或更高(n=4,OR 1.46(0.73-2.16),排除离群值)概率(P=42.0%和 89.3%)相关。低剂量试验(<1000mg 氢化可的松/天)与较低的死亡率概率相关(n=9,OR 0.80(0.40-1.39);n=8,OR 0.71(0.37-1.10),排除离群值)(分别为 20.4%和 5.8%)。低剂量试验中休克缓解的 OR 增加(n=7;OR 1.20(1.07-4.55);P=98.2%)。皮质激素对促皮质素刺激的反应性不是决定性的。在低剂量试验中,通过荟萃回归确定了与风险相关的治疗效果的高概率(随着对照臂风险的增加,对数优势死亡率的降低)(n=9,斜率系数-0.49(-1.14,0.27);P=92.2%)。皮质激素治疗并没有增加并发症的几率。
虽然不能排除低剂量皮质类固醇治疗严重脓毒症和败血症性休克的死亡率治疗效果为零,但仍有很高的治疗效果概率,排除离群值后更是如此。同样,虽然不能排除低剂量类固醇的有利作用,但低剂量类固醇的有利作用很可能依赖于患者的基础风险。皮质激素在促皮质素无反应者中未显示出疗效。似乎需要进行进一步的大规模试验。