Villavicencio Alan T, Burneikiene Sigita, Roeca Cassandra M, Nelson E Lee, Mason Alexander
Boulder Neurosurgical Associates, Boulder, CO; USA.
Surg Neurol Int. 2010 May 31;1:12. doi: 10.4103/2152-7806.63905.
Available clinical data are insufficient for comparing minimally invasive (MI) and open approaches for transforaminal lumbar interbody fusion (TLIF). To date, a paucity of literature exists directly comparing minimally invasive (MI) and open approaches for transforaminal lumbar interbody fusion (TLIF). The purpose of this study was to directly compare safety and effectiveness for these two surgical approaches.
Open or minimally invasive TLIF was performed in 63 and 76 patients, respectively. All consecutive minimally invasive TLIF cases were matched with a comparable cohort of open TLIF cases using three variables: diagnosis, number of spinal levels, and history of previous lumbar surgery. Patients were treated for painful degenerative disc disease with or without disc herniation, spondylolisthesis, and/or stenosis at one or two spinal levels. Clinical outcome (self-report measures, e.g., visual analog scale (VAS), patient satisfaction, and MacNab's criteria), operative data (operative time, estimated blood loss), length of hospitalization, and complications were assessed. Average follow-up for patients was 37.5 months.
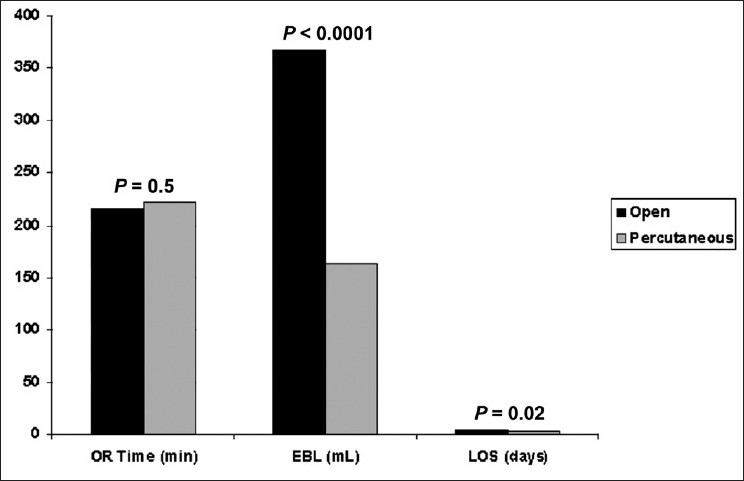
The mean change in VAS scores postoperatively was greater (5.2 vs. 4.1) in theopen TLIF patient group (P = 0.3). MacNab's criteria score was excellent/good in 67% and 70% (P = 0.8) of patients in open and minimally invasive TLIF groups, respectively. The overall patient satisfaction was 72.1% and 64.5% (P = 0.4) in open and minimally invasive TLIF groups, respectively. The total mean operative time was 214.9 min for open and 222.5 min for minimally invasive TLIF procedures (P = 0.5). The mean estimated blood loss for minimally invasive TLIF (163.0 ml) was significantly lower (P < 0.0001) than the open approach (366.8 ml). The mean duration of hospitalization in the minimally invasive TLIF (3 days) was significantly shorter (P = 0.02) than the open group (4.2 days). The total rate of neurological deficit was 10.5% in the minimally invasive TLIF group compared to 1.6% in the open group (P = 0.02).
Minimally invasive TLIF technique may provide equivalent long-term clinical outcomes compared to open TLIF approach in select population of patients. The potential benefit of minimized tissue disruption, reduced blood loss, and length of hospitalization must be weighted against the increased rate of neural injury-related complications associated with a learning curve.
现有的临床数据不足以比较经椎间孔腰椎椎体间融合术(TLIF)的微创(MI)和开放手术方式。迄今为止,直接比较经椎间孔腰椎椎体间融合术(TLIF)的微创(MI)和开放手术方式的文献较少。本研究的目的是直接比较这两种手术方式的安全性和有效性。
分别对63例和76例患者实施了开放或微创TLIF手术。所有连续的微创TLIF病例与一组具有可比性的开放TLIF病例在三个变量上进行匹配:诊断、脊柱节段数和既往腰椎手术史。患者因一个或两个脊柱节段的疼痛性退行性椎间盘疾病伴或不伴椎间盘突出、椎体滑脱和/或椎管狭窄而接受治疗。评估临床结果(自我报告指标,如视觉模拟量表(VAS)、患者满意度和MacNab标准)、手术数据(手术时间、估计失血量)、住院时间和并发症。患者的平均随访时间为37.5个月。
开放TLIF患者组术后VAS评分的平均变化更大(5.2对4.1)(P = 0.3)。开放和微创TLIF组中分别有67%和70%的患者MacNab标准评分优秀/良好(P = 0.8)。开放和微创TLIF组患者的总体满意度分别为72.1%和64.5%(P = 0.4)。开放TLIF手术的总平均手术时间为214.9分钟,微创TLIF手术为222.5分钟(P = 0.5)。微创TLIF的平均估计失血量(163.0毫升)明显低于开放手术方式(366.8毫升)(P < 0.0001)。微创TLIF组的平均住院时间(3天)明显短于开放组(4.2天)(P = 0.02)。微创TLIF组神经功能缺损的总发生率为10.5%,而开放组为1.6%(P = 0.02)。
在特定患者群体中,与开放TLIF手术方式相比,微创TLIF技术可能提供相当的长期临床结果。必须在组织破坏最小化、失血量减少和住院时间缩短的潜在益处与学习曲线相关的神经损伤相关并发症发生率增加之间进行权衡。