Simard Edgar P, Pfeiffer Ruth M, Engels Eric A
Infections and Immunoepidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, 6120 Executive Blvd, EPS 7076, Rockville, MD 20892, USA.
Arch Intern Med. 2010 Aug 9;170(15):1337-45. doi: 10.1001/archinternmed.2010.253.
Persons living with AIDS today remain at elevated cancer risk. Highly active antiretroviral therapy (HAART), widely available since 1996, prolongs life, but immune function is not fully restored. We conducted this study to assess long-term cancer risk among persons with AIDS relative to the general population and the impact of HAART on cancer incidence.
Records of 263 254 adults and adolescents with AIDS (1980-2004) from 15 US regions were matched to cancer registries to capture incident cancers during years 3 through 5 and 6 through 10 after AIDS onset. Standardized incidence ratios (SIRs) were used to assess risks relative to the general population. Rate ratios (RRs) were used to compare cancer incidence before and after 1996 to assess the impact of availability of HAART.
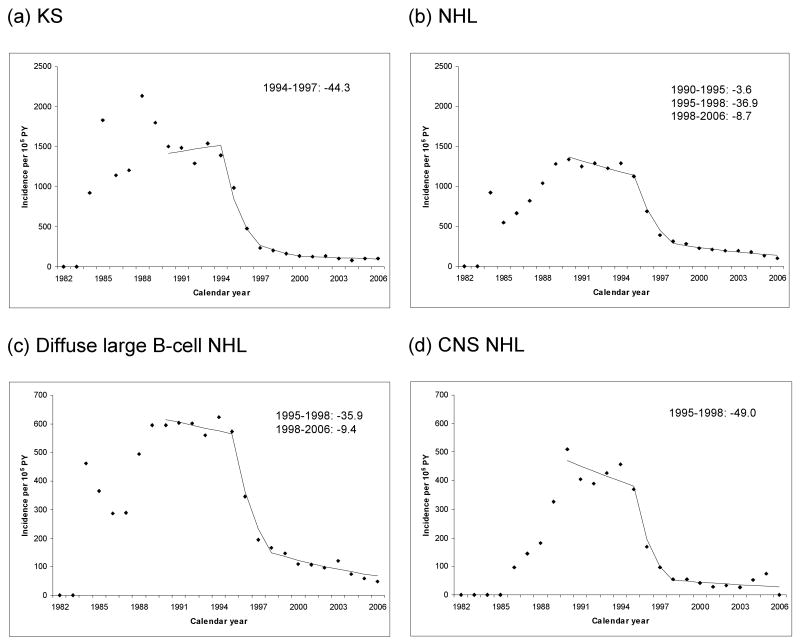
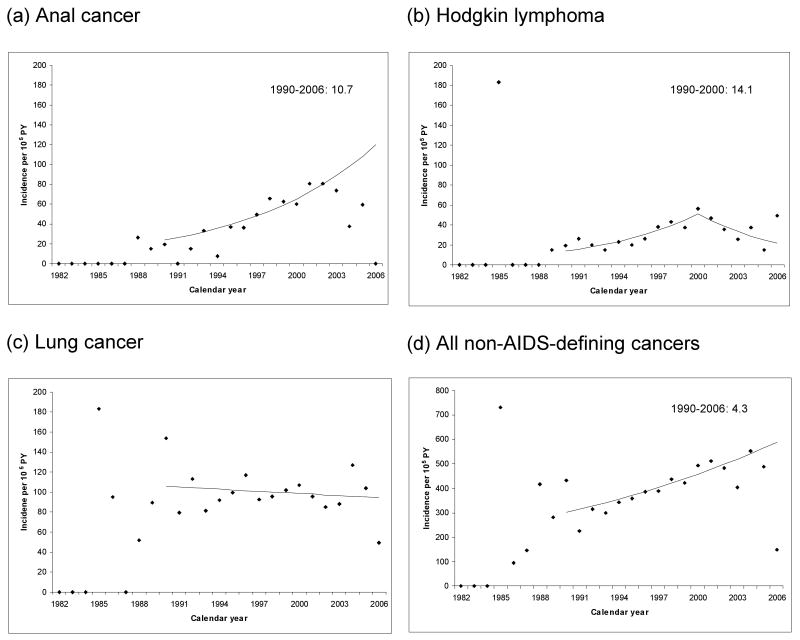
Risk was elevated for the 2 major AIDS-defining cancers: Kaposi sarcoma (SIRs, 5321 and 1347 in years 3-5 and 6-10, respectively) and non-Hodgkin lymphoma (SIRs, 32 and 15). Incidence of both malignancies declined in the HAART era (1996-2006). Risk was elevated for all non-AIDS-defining cancers combined (SIRs, 1.7 and 1.6 in years 3-5 and 6-10, respectively) and for the following specific non-AIDS-defining cancers: Hodgkin lymphoma and cancers of the oral cavity and/or pharynx, tongue, anus, liver, larynx, lung and/or bronchus, and penis. Anal cancer incidence increased between 1990-1995 and 1996-2006 (RR, 2.9; 95% confidence interval [CI], 2.1-4.0), as did that of Hodgkin lymphoma (RR, 2.0; 95% CI, 1.3-2.9).
Among people who survived for several years or more after an AIDS diagnosis, we observed high risks of AIDS-defining cancers and increasing incidence of anal cancer and Hodgkin lymphoma.
如今,艾滋病患者仍面临着更高的患癌风险。自1996年广泛应用以来,高效抗逆转录病毒疗法(HAART)延长了患者的生命,但免疫功能并未完全恢复。我们开展这项研究,旨在评估艾滋病患者相对于普通人群的长期患癌风险以及HAART对癌症发病率的影响。
将来自美国15个地区的263254名成人及青少年艾滋病患者(1980 - 2004年)的记录与癌症登记处进行匹配,以获取艾滋病发病后第3至5年以及第6至10年期间的新发癌症病例。标准化发病比(SIRs)用于评估相对于普通人群的风险。率比(RRs)用于比较1996年前后的癌症发病率,以评估HAART的应用所产生的影响。
两种主要的艾滋病定义性癌症风险升高:卡波西肉瘤(第3至5年和第6至10年的SIRs分别为5321和1347)以及非霍奇金淋巴瘤(SIRs分别为32和15)。在HAART时代(1996 - 2006年),这两种恶性肿瘤的发病率均有所下降。所有非艾滋病定义性癌症合并后的风险升高(第3至5年和第6至10年的SIRs分别为1.7和1.6),以下特定的非艾滋病定义性癌症风险也升高:霍奇金淋巴瘤以及口腔和/或咽部、舌、肛门、肝脏、喉、肺和/或支气管、阴茎的癌症。1990 - 1995年至1996 - 2006年期间,肛门癌发病率增加(RR,2.9;95%置信区间[CI],2.1 - 4.0),霍奇金淋巴瘤发病率也增加(RR,2.0;95%CI,1.3 - 2.9)。
在艾滋病诊断后存活数年或更长时间的人群中,我们观察到艾滋病定义性癌症的高风险以及肛门癌和霍奇金淋巴瘤发病率的增加。