Department of Biostatistics and Bioinformatics, Emory University School of Public Health, Atlanta, GA, USA.
BMC Infect Dis. 2010 Aug 25;10:254. doi: 10.1186/1471-2334-10-254.
Using mathematical deterministic models of the epidemiology of hospital-acquired infections and antibiotic resistance, it has been shown that the rates of hospital-acquired bacterial infection and frequency of antibiotic infections can be reduced by (i) restricting the admission of patients colonized with resistant bacteria, (ii) increasing the rate of turnover of patients, (iii) reducing transmission by infection control measures, and (iv) the use of second-line drugs for which there is no resistance. In an effort to explore the generality and robustness of the predictions of these deterministic models to the real world of hospitals, where there is variation in all of the factors contributing to the incidence of infection, we developed and used a stochastic model of the epidemiology of hospital-acquired infections and resistance. In our analysis of the properties of this model we give particular consideration different regimes of using second-line drugs in this process.
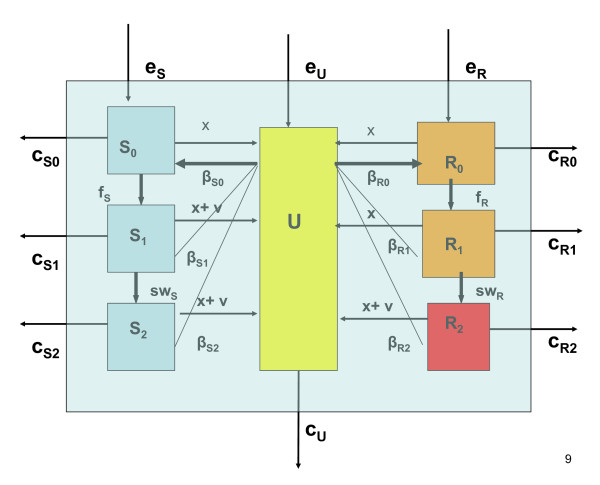
We developed a simple model that describes the transmission of drug-sensitive and drug-resistant bacteria in a small hospital. Colonized patients may be treated with a standard drug, for which there is some resistance, and with a second-line drug, for which there is no resistance. We then ran deterministic and stochastic simulation programs, based on this model, to predict the effectiveness of various treatment strategies.
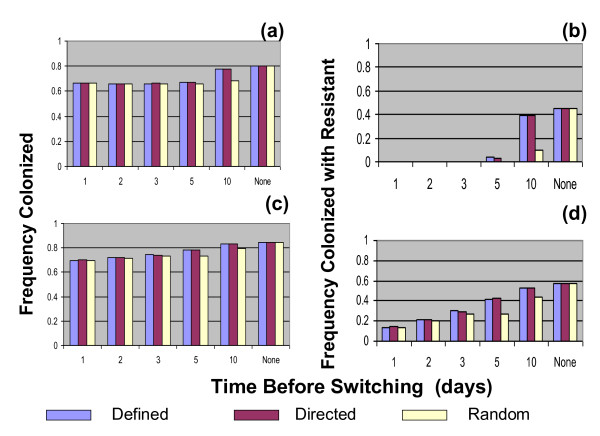
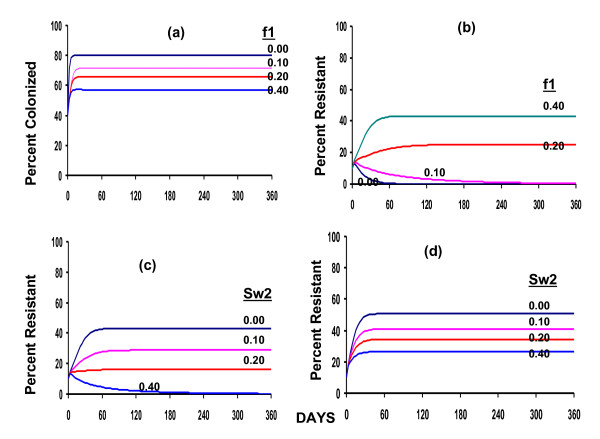
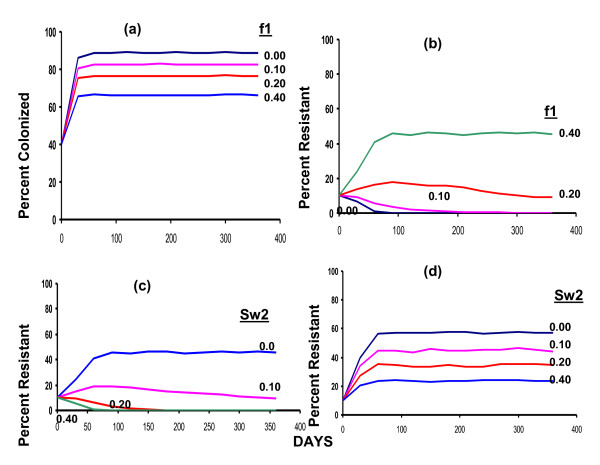
The results of the analysis using our stochastic model support the predictions of the deterministic models; not only will the implementation of any of the above listed measures substantially reduce the incidences of hospital-acquired infections and the frequency of resistance, the effects of their implementation should be seen in months rather than the years or decades anticipated to control resistance in open communities. How effectively and how rapidly the application of second-line drugs will contribute to the decline in the frequency of resistance to the first-line drugs depends on how these drugs are administered. The earlier the switch to second-line drugs, the more effective this protocol will be. Switching to second-line drugs at random is more effective than switching after a defined period or only after there is direct evidence that the patient is colonized with bacteria resistant to the first antibiotic.
The incidence of hospital-acquired bacterial infections and frequencies of antibiotic resistant bacteria can be markedly and rapidly reduced by different readily implemented procedures. The efficacy using second line drugs to achieve these ends depends on the protocol used for their administration.
通过对医院获得性感染和抗生素耐药性的流行病学进行数学确定性建模,已经表明可以通过以下方式降低医院获得性细菌感染的发生率和抗生素感染的频率:(i)限制耐药菌定植患者的入院,(ii)提高患者周转率,(iii)通过感染控制措施减少传播,以及(iv)使用无耐药性的二线药物。为了探索这些确定性模型对医院实际情况的预测的普遍性和稳健性,因为在所有导致感染发生率的因素中都存在变化,我们开发并使用了医院获得性感染和耐药性的流行病学随机模型。在对该模型特性的分析中,我们特别考虑了在该过程中使用二线药物的不同方案。
我们开发了一个简单的模型,描述了在一家小型医院中耐药和敏感细菌的传播。定植患者可以接受标准药物治疗,该药物有一定的耐药性,也可以接受二线药物治疗,该药物无耐药性。然后,我们根据该模型运行确定性和随机模拟程序,预测各种治疗策略的有效性。
使用我们的随机模型进行的分析结果支持确定性模型的预测;上述措施的实施不仅将大大降低医院获得性感染的发生率和耐药菌的频率,而且其实施效果将在数月内显现,而不是像控制开放社区耐药性那样需要数年或数十年。二线药物的应用将如何有效地快速降低对一线药物的耐药频率,取决于这些药物的使用方式。越早切换到二线药物,该方案就越有效。随机切换到二线药物比在规定时间后或只有在有直接证据表明患者定植了对第一种抗生素耐药的细菌后切换更有效。
通过不同的易于实施的程序,可以显著且快速地降低医院获得性细菌感染的发生率和抗生素耐药菌的频率。使用二线药物实现这些目标的疗效取决于用于管理这些药物的方案。