Department of Radiology, St Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, Kanagawa 216-8511, Japan.
Arthritis Res Ther. 2010;12(5):R171. doi: 10.1186/ar3131. Epub 2010 Sep 13.
Rheumatoid arthritis (RA) is a multi-organ inflammatory disorder associated with high cardiovascular morbidity and mortality. We sought to assess cardiac involvement using a comprehensive cardiac magnetic resonance imaging (cMRI) approach and to determine its association with disease characteristics in RA patients without symptomatic cardiac disease.
RA patients with no history and/or clinical findings of systemic or pulmonary hypertension, coronary artery disease, severe valvular heart disease, atrial fibrillation, diabetes mellitus, or echocardiographic abnormalities underwent contrast-enhanced cMRI on a 1.5T scanner. Adenosine triphosphate was used to assess perfusion defects due to microvascular impairment or ischemia, and delayed enhanced imaging was obtained for the assessment of myocardial inflammation/fibrosis. We explored the associations of cMRI abnormalities with RA disease activity and severity measures.
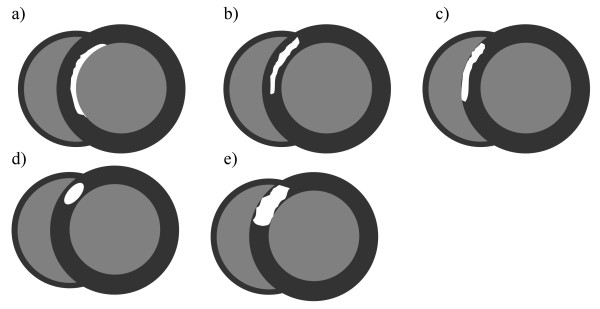
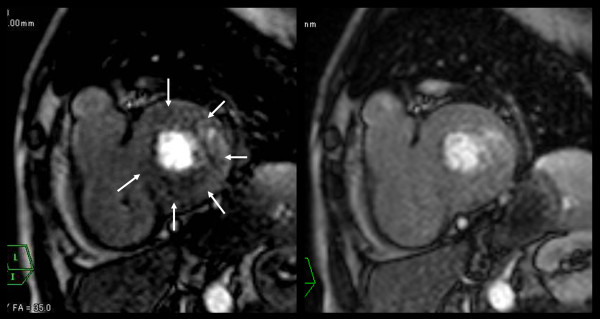
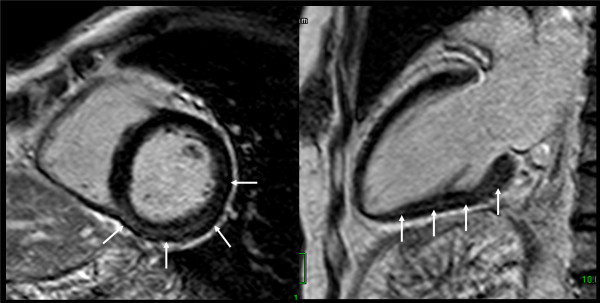
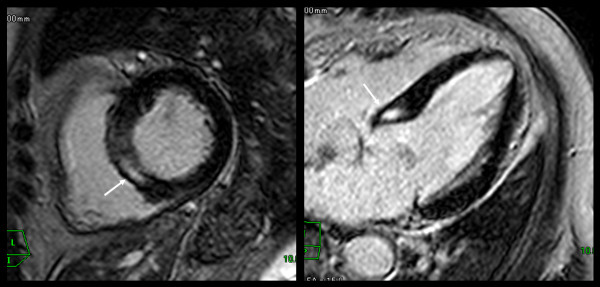
Eighteen patients (78% female) with a mean age of 57 ± 10 years were studied. Eight patients (45%) demonstrated a myocardial abnormality. Perfusion defects under pharmacologic stress were seen in two patients (11%), one of whom had a circumferential subendocardial perfusion defect and one had a non-segmental subendocardial perfusion defect. Seven patients (39%) were found to have delayed enhancement, only one of whom also demonstrated a perfusion defect. Mean disease activity score (DAS)28 was significantly higher in the group with delayed enhancement compared to the group without by an average of 1.32 DAS28 units (4.77 vs. 3.44 units, respectively; P = 0.011). Corresponding trends to statistical significance were noted in systemic inflammatory markers, with both C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) quantitatively higher in the group with delayed enhancement. Other RA characteristics, such as disease duration, autoantibody status, and current treatments were not significantly associated with cardiac involvement.
Myocardial abnormalities, as detected by cMRI, were frequent in RA patients without known cardiac disease. Abnormal cMRI findings were associated with higher RA disease activity, suggesting a role for inflammation in the pathogenesis of myocardial involvement in RA.
类风湿关节炎(RA)是一种多器官炎症性疾病,与心血管发病率和死亡率高有关。我们试图通过综合心脏磁共振成像(cMRI)方法评估心脏受累情况,并确定其与无症状性心脏疾病的 RA 患者的疾病特征之间的关联。
无系统性或肺动脉高压、冠状动脉疾病、严重瓣膜性心脏病、心房颤动、糖尿病或超声心动图异常病史和/或临床发现的 RA 患者接受了 1.5T 扫描仪上的对比增强 cMRI。三磷酸腺苷(adenosine triphosphate)用于评估微血管损伤或缺血引起的灌注缺陷,延迟增强成像用于评估心肌炎症/纤维化。我们探讨了 cMRI 异常与 RA 疾病活动和严重程度指标的相关性。
研究了 18 名(78%为女性)平均年龄为 57±10 岁的患者。8 名患者(45%)存在心肌异常。两名患者(11%)出现药物应激下的灌注缺陷,其中一名患者存在环形心内膜下灌注缺陷,另一名患者存在非节段性心内膜下灌注缺陷。7 名患者(39%)出现延迟强化,其中只有 1 名患者同时存在灌注缺陷。与无延迟强化组相比,延迟强化组的平均疾病活动评分(DAS)28 显著升高,平均升高 1.32 DAS28 单位(分别为 4.77 和 3.44 单位;P=0.011)。在系统性炎症标志物中也观察到了统计学意义上的趋势,延迟强化组的 C 反应蛋白(CRP)和红细胞沉降率(ESR)均定量升高。其他 RA 特征,如疾病持续时间、自身抗体状态和当前治疗方案与心脏受累无显著相关性。
在无已知心脏疾病的 RA 患者中,通过 cMRI 检测到的心肌异常较为常见。异常的 cMRI 发现与 RA 疾病活动度较高相关,提示炎症在 RA 心肌受累的发病机制中起作用。