Mack Jennifer W, Paulk M Elizabeth, Viswanath Kasisomayajula, Prigerson Holly G
Department of Pediatric Oncology and Center for Outcomes and Policy Research, Dana-Farber Cancer Institute, Boston, Massachusetts 02115, USA.
Arch Intern Med. 2010 Sep 27;170(17):1533-40. doi: 10.1001/archinternmed.2010.322.
Black patients tend to receive more life-prolonging care at the end of life (EOL) than white patients. This study aimed to evaluate whether differences in patient-physician communication contribute to disparities in EOL care between black patients and white patients.
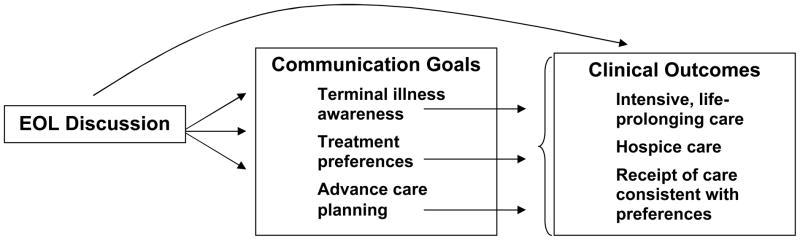
Multi-institutional prospective longitudinal cohort study of 71 black patients and 261 white patients with advanced cancer. The main outcome measures were differences between black patients and white patients in relationships among EOL discussions and communication goals (terminal illness awareness, treatment preferences, and do-not-resuscitate [DNR] orders) and EOL care outcomes (life-prolonging care, hospice care, and receipt of EOL care consistent with preferences).
End-of-life discussions between physicians and their white patients were associated with less life-prolonging EOL care compared with their black patients (adjusted odds ratio [aOR], 0.11; P = .04). Despite similar rates of EOL discussions (black vs white patients 35.3% vs 38.4%, P = .65), more black patients than white patients received life-prolonging EOL care (19.7% vs 6.9%, P = .001). End-of-life discussions were associated with attainment of some communication goals among black patients, including placement of DNR orders (aOR, 4.25; P = .04), but these communication goals were not consistently associated with EOL care received by black patients. For example, black patients with DNR orders were no less likely than black patients without DNR orders to receive life-prolonging EOL care (aOR, 1.57; P = .58).
End-of-life discussions and communication goals seem to assist white patients in receiving less life-prolonging EOL care, but black patients do not experience the same benefits of EOL discussions. Instead, black patients tend to receive life-prolonging measures at the EOL even when they have DNR orders or state a preference for symptom-directed care.
与白人患者相比,黑人患者在生命终末期(EOL)往往接受更多的延长生命治疗。本研究旨在评估医患沟通差异是否导致黑人患者与白人患者在生命终末期治疗上的差异。
对71名患有晚期癌症的黑人患者和261名白人患者进行多机构前瞻性纵向队列研究。主要结局指标是黑人患者与白人患者在生命终末期讨论与沟通目标(终末期疾病认知、治疗偏好和不进行心肺复苏[DNR]医嘱)之间的关系,以及生命终末期治疗结局(延长生命治疗、临终关怀和接受符合偏好的生命终末期治疗)的差异。
与黑人患者相比,医生与白人患者进行的生命终末期讨论与较少的延长生命的生命终末期治疗相关(调整后的优势比[aOR],0.11;P = 0.04)。尽管生命终末期讨论的比例相似(黑人患者与白人患者分别为35.3%和38.4%,P = 0.65),但接受延长生命的生命终末期治疗的黑人患者比白人患者更多(19.7%对6.9%,P = 0.001)。生命终末期讨论与黑人患者实现一些沟通目标相关,包括下达DNR医嘱(aOR,4.25;P = 0.04),但这些沟通目标与黑人患者接受的生命终末期治疗并不始终相关。例如,有DNR医嘱的黑人患者接受延长生命的生命终末期治疗的可能性并不低于没有DNR医嘱的黑人患者(aOR,1.57;P = 0.58)。
生命终末期讨论和沟通目标似乎有助于白人患者接受较少的延长生命的生命终末期治疗,但黑人患者并未从生命终末期讨论中获得同样的益处。相反,黑人患者在生命终末期往往接受延长生命的措施,即使他们有DNR医嘱或表示倾向于以症状为导向的治疗。