Department of Clinical Nursing Science, School of Health and Society, Kristianstad University, Kristianstad, Sweden.
Food Nutr Res. 2010 Sep 24;54:5402. doi: 10.3402/fnr.v54i0.5402.
Disease-related malnutrition is a major health problem in the elderly population and management issues are under-explored.
What is the prevalence of undernutrition-risk (UN-risk), underweight, and overweight in special accommodations (SAs)? Do study circles and a nutritional care policy (NCP) improve the precision in nutritional care (NC) and decrease the prevalence of under- and overweight in a short- and/or long-term perspective?
Quasi-experimental pre- and post-intervention design with three experimental groups and one control group (CG).
SAs.
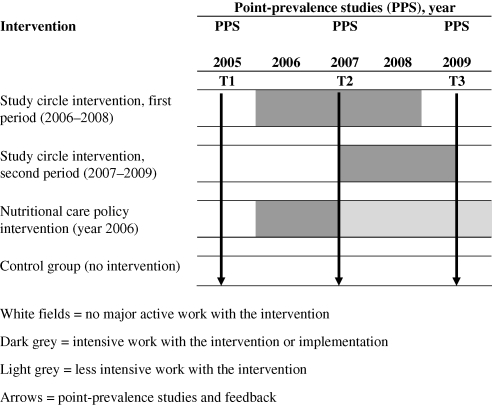
In 2005 (Time 1 - T1), 1726 (90.4%) residents agreed to participate; in 2007 (Time 2 - T2), 1,526 (81.8%); and in 2009 (Time 3 - T3), 1,459 (81.3%) residents participated.
between T1 and T2 the first period of study circles was conducted in one municipality; between T2 and T3 a second period of study circles in another municipality was conducted; after T1 a NCP was implemented in one municipality. CG: residents in three municipalities.
Under- and overweight were defined based on BMI. Risk of undernutrition was defined as involving any of: involuntary weight loss, low BMI, and/or eating difficulties. The 'precision in NC' describes the relationship between nutritional treatment (protein- and energy-enriched food (PE-food) and/or oral supplements) and UN-risk.
The prevalence of UN-risk varied between 64 and 66%, underweight between 25 and 30%, and overweight between 30 and 33% in T1-T3. At T2 the prevalence of underweight was significantly lower in the first period study circle municipality, and at T3 in the second period study circle municipality compared to in the CG. The precision in NC was higher in a short-term perspective in the study circle municipalities and both in a short- and long-term perspective in the NCP municipality. At T3 between 54 and 70% of residents at UN-risk did not receive PE-food or oral supplements.
Study circles give positive short-term effects and a NCP gives positive short- and long-term effects on NC. Whether a combination of study circles and the implementation of a NCP can give even better results is an area for future studies.
与疾病相关的营养不良是老年人群体中的一个主要健康问题,但其管理问题仍未得到充分探讨。
特殊住宿(SA)中营养风险(UN 风险)、体重不足和超重的患病率是多少?研究圈和营养护理政策(NCP)是否能提高营养护理(NC)的准确性,并在短期和/或长期内降低低体重和超重的患病率?
具有三个实验组和一个对照组(CG)的准实验前后干预设计。
SA。
2005 年(时间 1-T1),1726 名(90.4%)居民同意参与;2007 年(时间 2-T2),1526 名(81.8%)居民参与;2009 年(时间 3-T3),1459 名(81.3%)居民参与。
在 T1 到 T2 之间,第一个研究圈期间在一个直辖市进行;在 T2 到 T3 之间,另一个直辖市进行了第二个研究圈期间;在 T1 之后,一个直辖市实施了 NCP。CG:三个直辖市的居民。
低体重和超重根据 BMI 定义。营养风险定义为:非自愿性体重减轻、低 BMI 和/或饮食困难。“NC 的准确性”描述了营养治疗(蛋白质和能量强化食品(PE-食品)和/或口服补充剂)与 UN 风险之间的关系。
T1-T3 期间,UN 风险的患病率在 64%至 66%之间,体重不足的患病率在 25%至 30%之间,超重的患病率在 30%至 33%之间。在 T2 时,第一个研究圈直辖市的体重不足患病率明显低于 CG,在 T3 时,第二个研究圈直辖市的体重不足患病率也明显低于 CG。在短期方面,研究圈直辖市的 NC 准确性更高,在短期和长期方面,NCP 直辖市的 NC 准确性更高。在 T3 时,54%至 70%的 UN 风险居民未接受 PE-食品或口服补充剂。
研究圈在短期内产生积极影响,NCP 在短期和长期内对 NC 产生积极影响。研究圈和 NCP 的结合是否能产生更好的结果,这是一个有待未来研究的领域。