Levi Dennis M, McKee Suzanne P, Movshon J Anthony
School of Optometry and Helen Wills Neuroscience Institute, University of California, Berkeley, CA 94720, USA.
Vision Res. 2011 Jan;51(1):48-57. doi: 10.1016/j.visres.2010.09.029. Epub 2010 Oct 7.
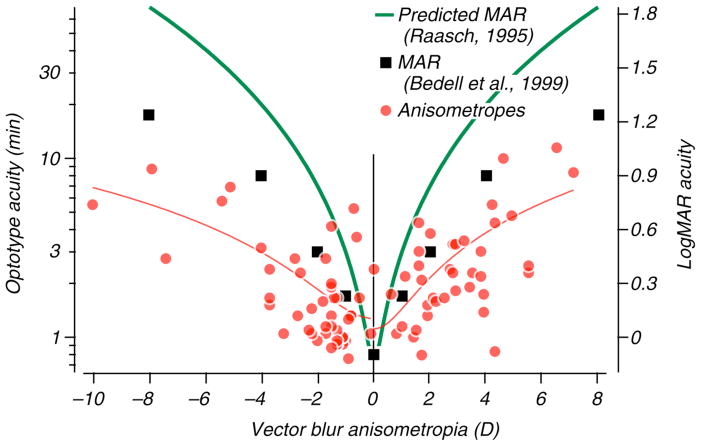
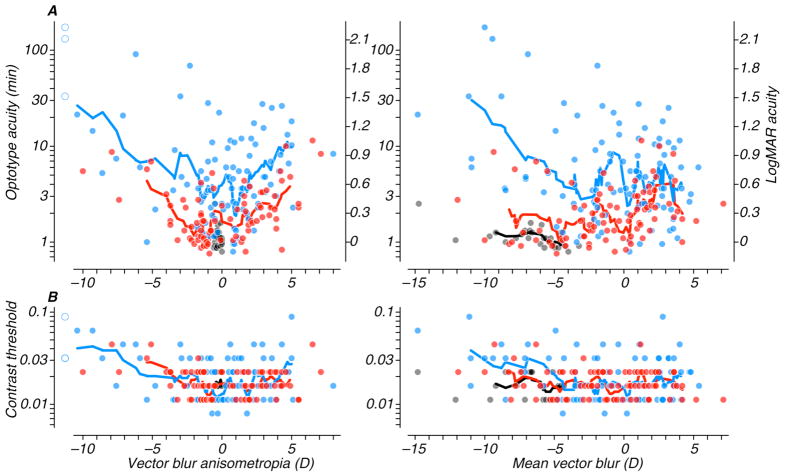
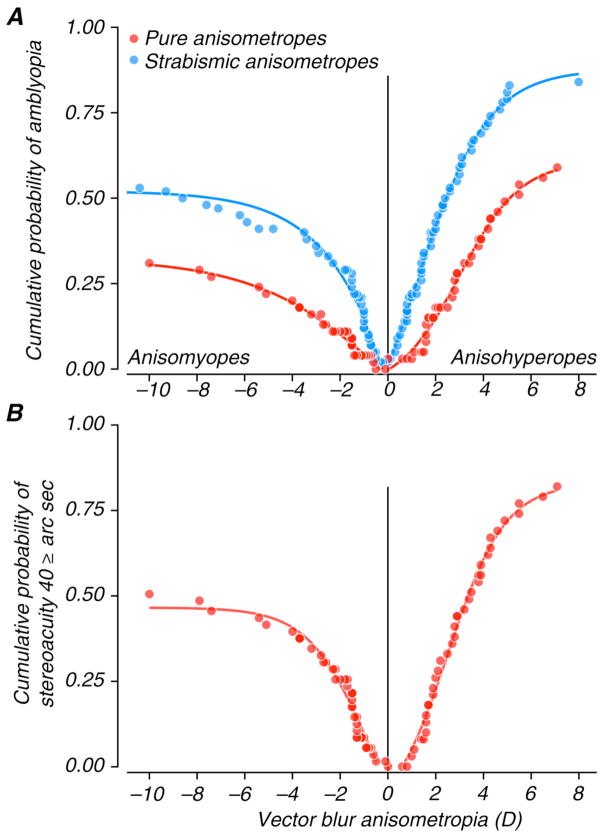
Amblyopia is usually associated with the presence of anisometropia, strabismus or both early in life. We set out to explore quantitative relationships between the degree of anisometropia and the loss of visual function, and to examine how the presence of strabismus affects visual function in observers with anisometropia. We measured optotype acuity, Pelli-Robson contrast sensitivity and stereoacuity in 84 persons with anisometropia and compared their results with those of 27 persons with high bilateral refractive error (isoametropia) and 101 persons with both strabismus and anisometropia. All subjects participated in a large-scale study of amblyopia (McKee et al., 2003). We found no consistent visual abnormalities in the strong eye, and therefore report only on vision in the weaker, defined as the eye with lower acuity. LogMAR acuity falls off markedly with increasing anisometropia in non-strabismic anisometropes, while contrast sensitivity is much less affected. Acuity degrades rapidly with increases in both hyperopic and myopic anisometropia, but the risk of amblyopia is about twice as great in hyperopic than myopic anisometropes of comparable refractive imbalance. For a given degree of refractive imbalance, strabismic anisometropes perform considerably worse than anisometropes without strabismus--visual acuity for strabismics was on average 2.5 times worse than for non-strabismics with similar anisometropia. For observers with equal refractive error in the two eyes there is very little change in acuity or sensitivity with increasing (bilateral) refractive error except for one extreme individual (bilaterally refractive error of -15 D). Most pure anisometropes with interocular differences less than 4D retain some stereopsis, and the degree is correlated with the acuity of the weak eye. We conclude that even modest interocular differences in refractive error can influence visual function.
弱视通常与生命早期存在的屈光参差、斜视或两者都有关。我们着手探索屈光参差程度与视觉功能丧失之间的定量关系,并研究斜视的存在如何影响屈光参差观察者的视觉功能。我们测量了84名屈光参差患者的视标视力、佩利-罗布森对比敏感度和立体视锐度,并将他们的结果与27名双眼高度屈光不正(等屈光不正)患者和101名既有斜视又有屈光参差患者的结果进行比较。所有受试者都参与了一项关于弱视的大规模研究(麦基等人,2003年)。我们在优势眼中未发现一致的视觉异常,因此仅报告较弱眼的视力,较弱眼定义为视力较低的眼睛。在非斜视性屈光参差患者中,最小分辨角对数视力随着屈光参差的增加而显著下降,而对比敏感度受影响较小。远视性和近视性屈光参差增加时,视力都会迅速下降,但在可比屈光不平衡的远视性屈光参差患者中,弱视风险约为近视性屈光参差患者的两倍。对于给定程度的屈光不平衡,斜视性屈光参差患者的表现明显比无斜视的屈光参差患者差——斜视患者的视力平均比具有相似屈光参差的非斜视患者差2.5倍。对于双眼屈光不正相等的观察者,除了一名极端个体(双眼屈光不正为-15 D)外,随着(双眼)屈光不正增加,视力或敏感度变化很小。大多数双眼差异小于4D的单纯屈光参差患者仍保留一定程度的立体视,且其程度与弱眼视力相关。我们得出结论,即使是屈光不正的微小双眼差异也会影响视觉功能。