Department of Pediatrics, Division of Gastroenterology and Nutrition, The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
Gastroenterology. 2011 Feb;140(2):450-458.e1. doi: 10.1053/j.gastro.2010.10.047. Epub 2010 Oct 28.
BACKGROUND & AIMS: Although randomized trials of adults infected with hepatitis C virus (HCV) have shown that ribavirin increases the efficacy of pegylated interferon (PEG), such trials have not been performed in children. We conducted a randomized controlled trial of PEG and ribavirin, compared with PEG and placebo, in children 5 to 17 years old with chronic hepatitis C.
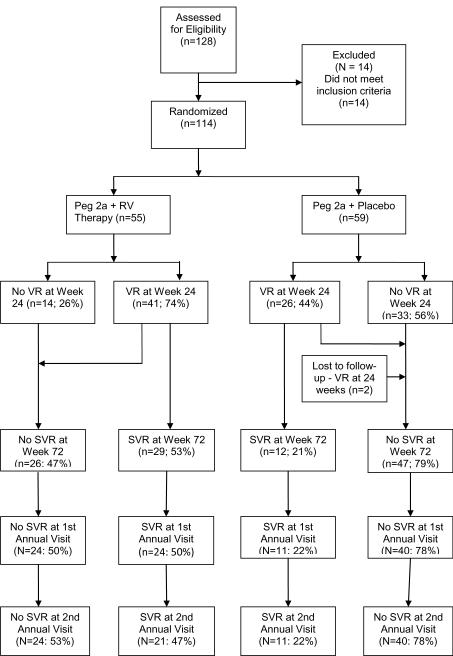
HCV RNA-positive children from 11 university medical centers were randomly assigned to receive either PEG alfa-2a (PEG-2a; 180 μg/1.73 m(2) body surface area, subcutaneously each week; n = 55) and ribavirin (15 mg/kg orally in 2 doses daily) or PEG-2a and placebo (n = 59) for 48 weeks. The primary end point was sustained virologic response (SVR; lack of detectable HCV RNA at least 24 weeks after stopping therapy).
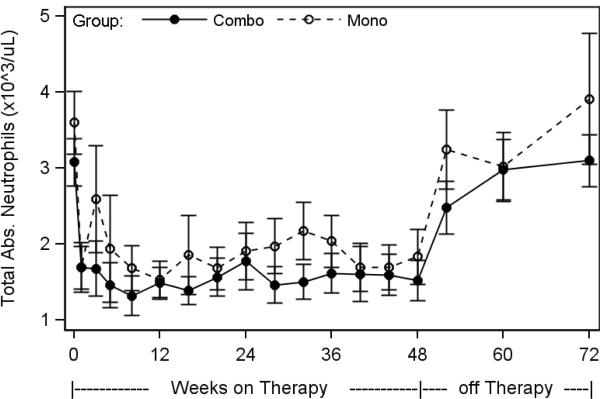
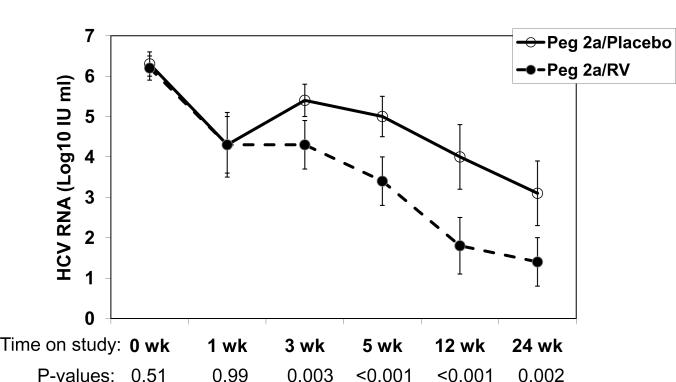
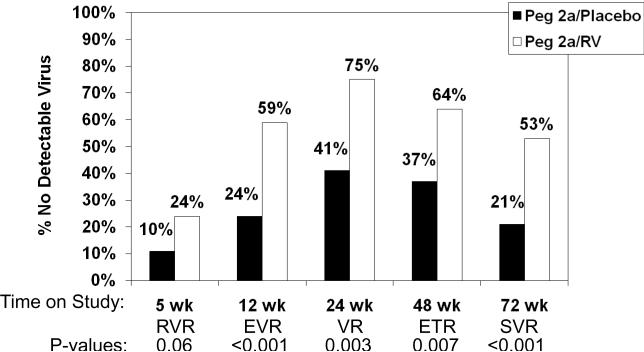
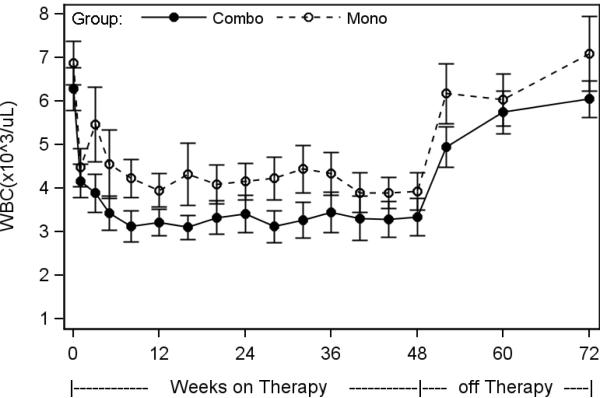
SVR was achieved in 53% of children treated with PEG-2a and ribavirin, compared with 21% of children who received PEG-2a and placebo (P < .001). Early virologic response (HCV RNA reduction >2 log(10) IU at 12 weeks) had a negative predictive value of only 0.89 in children with genotype 1, indicating that these children might benefit from 24 weeks of therapy before stopping treatment. Side effects, especially neutropenia, led to dose modification in 40% of children. Eighty-two percent of the PEG/ribavirin and 86% of the PEG/placebo group were in compliance with the year 2 follow-up visit; the durability of virologic response was 100% in both groups.
The combination of PEG and ribavirin is superior to PEG and placebo as therapy for chronic hepatitis C in children and adolescents.
虽然针对感染丙型肝炎病毒(HCV)的成人进行的随机试验表明,利巴韦林可提高聚乙二醇干扰素(PEG)的疗效,但此类试验并未在儿童中进行。我们对 5 至 17 岁慢性丙型肝炎儿童进行了 PEG 和利巴韦林的随机对照试验,与 PEG 和安慰剂进行了比较。
来自 11 所大学医学中心的 HCV RNA 阳性儿童被随机分配接受 PEG 阿尔法-2a(PEG-2a;180μg/1.73m² 体表面积,皮下每周一次;n=55)和利巴韦林(15mg/kg 分两次口服,每日 2 次)或 PEG-2a 和安慰剂(n=59)治疗 48 周。主要终点是持续病毒学应答(SVR;停药后至少 24 周时无法检测到 HCV RNA)。
接受 PEG-2a 和利巴韦林治疗的儿童中,有 53%实现了 SVR,而接受 PEG-2a 和安慰剂治疗的儿童中,只有 21%实现了 SVR(P<.001)。对于基因型 1 的儿童,早期病毒学应答(12 周时 HCV RNA 降低>2 log10IU)的阴性预测值仅为 0.89,表明这些儿童可能受益于治疗 24 周后再停止治疗。副作用,特别是中性粒细胞减少症,导致 40%的儿童需要调整剂量。PEG/利巴韦林组和 PEG/安慰剂组分别有 82%和 86%的儿童符合随访 1 年的要求;两组的病毒学应答持久性均为 100%。
PEG 和利巴韦林联合治疗儿童和青少年慢性丙型肝炎优于 PEG 和安慰剂。